No products in the cart.

Conductive education is a coherent system developed for people with neuromusculoskeletal and motor disorders. The approach centres on teaching children and adults how to manage movement difficulties through an integrated learning process that addresses both physical and cognitive aspects.
Rather than separating physical therapy, occupational therapy and education, conductive education combines these elements into a single program. A specially trained professional — the conductor — guides learners through structured activities known as task series, designed to build functional abilities progressively.
The core principle is active participation. Learners are encouraged to plan, attempt and complete each movement consciously, developing motor skills and cognitive strategies together.
Several principles distinguish conductive education from other interventions; each has a clear practical implication for families and clinicians:
Conventional therapy typically separates roles: physiotherapists address movement, occupational therapists focus on daily living skills and educators manage learning. Each discipline contributes valuable expertise, but sessions are often discrete and task-specific.
By contrast, conductive education integrates these domains within a single daily programme. The same conductor supports movement, education and skill development throughout sessions, reflecting the interconnected nature of everyday functioning.
The environment also differs. Rather than treatment tables and isolated exercises, conductive education uses adapted furniture and equipment arranged to encourage active problem-solving so that learners discover functional solutions themselves.
The conductor acts as educator, facilitator and coordinator. Training combines pedagogical methods with understanding of motor disorders so conductors can design task series and adapt facilitation to each learner’s needs.
Conductors do not perform tasks for learners; instead they create situations that enable independent success, observe performance closely and adjust programmes as abilities change.
Most conductors work with groups, managing individual requirements while using group processes to motivate and model behaviour. This balance requires specialised skill and continuous assessment of progress.
The question of whether conductive education qualifies as therapy prompts regular discussion among clinicians and families. Clarifying this distinction helps set realistic expectations about goals, methods and outcomes.
Traditional therapy generally follows a medical model: clinicians diagnose impairments, provide targeted treatments and measure progress against clinical markers. Interventions tend to focus on correcting specific deficits.
Conductive education is framed within an educational model. It treats motor difficulties as learning challenges and places emphasis on teaching functional strategies. The focus moves from treating a patient to supporting a learner to develop skills and independence.
The practical difference matters. In a medical therapy session, the professional may perform techniques or guide isolated exercises; the recipient can be relatively passive.
Conductive education requires active engagement. Learners are encouraged to plan and execute movements, to problem-solve and to generalise skills across daily activities. The conductor’s role is to design learning opportunities rather than to deliver treatment in the clinical sense.
The setting reflects these principles. Educational spaces are arranged with adapted furniture and task-focused equipment to promote functional activity, rather than standard clinical treatment tables.
Conductive education can either complement or, in some cases, operate alongside traditional therapies. Whether it replaces or supplements existing services depends on individual needs, local provision and professional advice.
Some centres provide standalone conductive education programmes; others work in partnership with physiotherapy, occupational therapy and speech and language therapy. In many cases, families benefit from a combined approach that addresses specific clinical issues while also supporting overall functioning and independence.
Families are advised to discuss local pathways with their healthcare team and with conductors to agree a coordinated plan that suits the individual’s goals and medical needs.

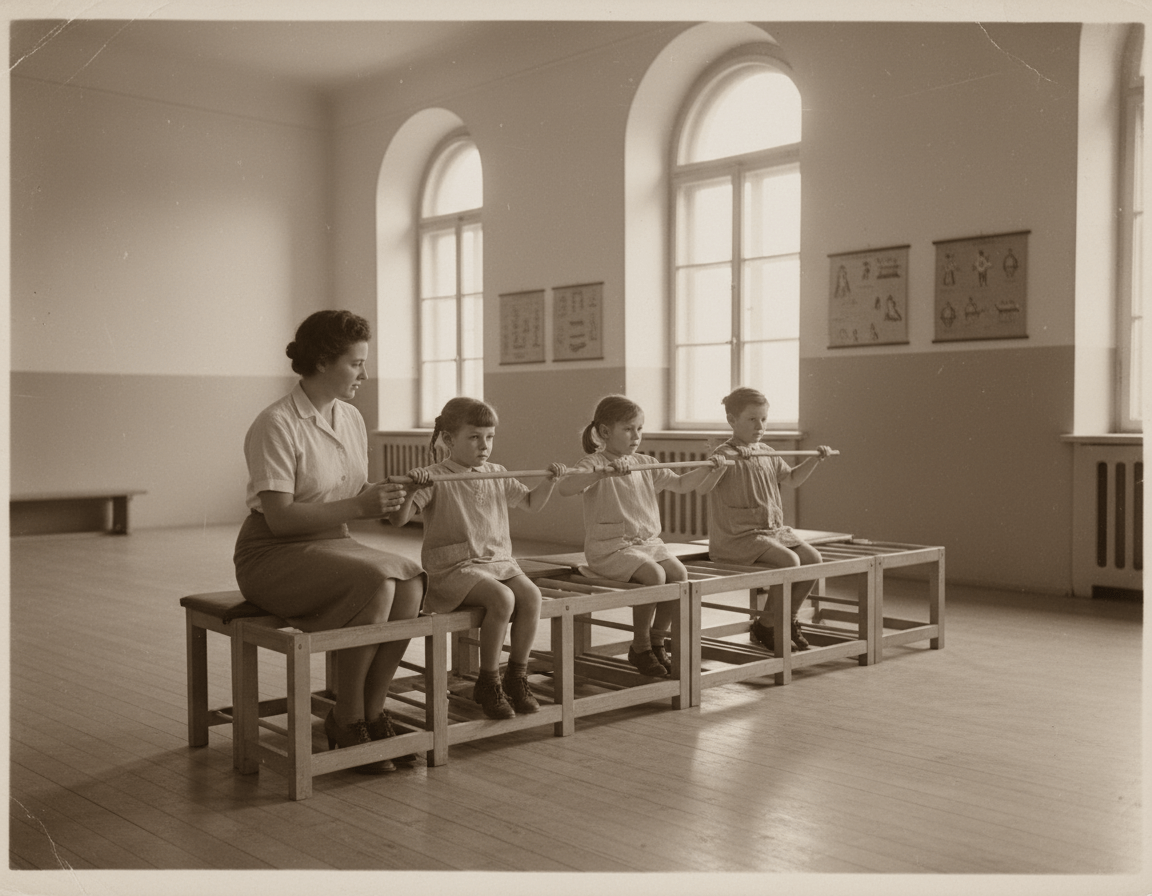
The origins of conductive education date to post‑World War II Hungary. Knowledge of its history helps explain the distinctive principles and practices used in the system today.
Dr András Pető, a Hungarian physician and educator, developed conductive education in the 1940s while working with children with cerebral palsy and adults with motor disorders. Pető observed that conventional medical treatments often produced limited functional change and proposed an alternative based on education and learning.
His approach reframed movement difficulties as problems of learning and organisation. The resulting system combined pedagogical methods with motor‑control principles to teach functional strategies rather than simply applying therapeutic techniques.
For several decades the method remained largely centred in Hungary. Political and practical barriers during the Cold War limited international exchange, so wider awareness developed only slowly.
Interest in the United Kingdom increased in the 1980s after British families and professionals visited Budapest and reported functional improvements. Early UK practitioners trained in Hungary returned to establish programmes that adapted Pető’s principles to British educational and healthcare settings.
Over the following decades conductive education grew steadily across the UK. Dedicated centres opened in England, Scotland, Wales and Northern Ireland, each tailoring programmes to local community needs while maintaining fidelity to core principles.
UK institutions began to offer conductor training, reducing reliance on overseas qualifications. Birmingham has been notable as a centre for professional development and training in the field.
Academic interest also increased. Research efforts examined outcomes, implementation and applications of conductive education across different populations. This scrutiny contributed to a gradually strengthening evidence base, while recognising that outcomes vary between individuals and programmes.
Families and healthcare professionals considering conductive education commonly ask what benefits can be expected. The approach targets multiple domains of functioning and development, with an emphasis on skills that transfer into daily life.
Motor skill development is a primary focus. Through systematic task series and the use of rhythmic intention, learners practise sequenced movements that support improved control and coordination.
Postural control frequently improves; specially designed furniture and structured activities encourage alignment and appropriate weight distribution, which supports function across everyday situations.
Balance and stability often show measurable gains. Practising within a group provides varied, dynamic challenges and peer models that reinforce motor learning beyond what isolated sessions typically achieve.
Conductive education integrates thinking with movement. Learners continuously plan, sequence and mentally rehearse actions, which strengthens executive functions such as planning and organisation.
Repeated practice within task series consolidates procedural learning and helps transfer skills into routine activities. Attention and concentration commonly improve in the structured, rhythmic group setting.
Group work supports personality development and reduces isolation. Working alongside peers facing comparable challenges fosters social skills, mutual encouragement and pragmatic communication.
Achieving functional goals typically builds self‑confidence. The emphasis on active problem‑solving encourages autonomy and a sense of competence rather than passive reliance on others.

Arguably the most important practical benefit is greater independence with routine activities. The functional focus means that practising transfers, dressing, eating and toileting within task series supports direct carry‑over to home and school.
Many families report that participants require less day‑to‑day assistance after sustained involvement in programmes. Outcomes are individual and depend on factors such as programme intensity, consistency of practice and family involvement.
Where clinical claims are made (for example, changes in spasticity or endurance), evidence varies between studies and between individuals; families and professionals should review outcome data from centres and consider realistic, person‑centred goals.
Deciding whether conductive education suits an individual requires consideration of clinical, developmental and practical factors. The approach is most appropriate where movement difficulties limit daily functioning and where the person can engage in an active learning process.
Conductive education was developed for children with cerebral palsy and has since been applied to a broader range of motor disorders. Typical indications include:
Conductive education serves individuals across the lifespan. Early intervention programmes for infants and toddlers aim to exploit neuroplasticity and establish foundational skills. School‑age provision combines educational and motor goals, using peer modelling to support development.
Adult programmes concentrate on maintaining and optimising function, maximising independence and reducing secondary complications. Programme goals and intensity are adapted to life roles and responsibilities at each stage.
A structured assessment by a qualified conductor will determine suitability. Key factors considered include:
Family involvement often enhances outcomes; when carers reinforce task series and routines at home, skills are more likely to carry over into daily life. Discussing local referral pathways with healthcare professionals and contacting centres for an initial consultation will help clarify whether conductive education meets individual needs.

Understanding how conductive education is delivered helps families prepare and allows professionals to integrate the approach into care plans. The methodology follows a structured process while remaining adaptable to each individual’s needs and abilities.
Task series form the backbone of conductive education sessions. Each series breaks a complex functional activity into ordered, practiceable components that build progressively towards the overall goal.
Typical goals include sitting independently, transferring from sit to stand, and walking with improved control. The conductor designs a task series after assessing the learner’s current ability and functional needs, then plans graded steps to achieve the goal.
Progression is scaffolded: simple components are practised first to establish reliable foundations before combining elements into more complex movements.
A standard task series usually comprises distinct, repeatable elements that together support skill learning:
The preparation phase readies body and mind. Activities may include positioning, gentle mobilisation, stretching and cognitive rehearsal of the upcoming actions.
Rhythmic intention often begins here: learners speak or chant short cues that describe the movement to be performed, linking intention with action.
During the active phase, the learner performs the planned movements with facilitation from the conductor. Support is reduced progressively as competence increases.
Group dynamics support this phase: observing peers provides models and encouragement, and the shared rhythm helps maintain timing and coordination.
Many conductive education programmes are intensive and structured across the day rather than offered as isolated short appointments. Intensive provision commonly includes multiple task series each day, allowing repeated practice and consolidation.
A typical day may focus on mobility and transfers in the morning and on fine motor skills or self‑care activities in the afternoon. Regular rest periods are scheduled to allow recovery without breaking the learning context, and social interaction at breaks reinforces group cohesion.
Specialist furniture and carefully arranged spaces support the educational process. Ladder‑back chairs offer graded trunk support, plinths facilitate positioning and parallel bars assist standing and gait practice.
Equipment is selected to encourage active problem‑solving: it provides sufficient assistance for safe practice while avoiding full support that would prevent the learner from devising their own movement solutions.
Environmental design—from floor surfaces to the placement of handrails—promotes independence by reducing unnecessary barriers to functional activity.

Contemporary programmes sometimes incorporate additional rehabilitation aids that align with conductive education principles. Any device used should promote active participation rather than create passive reliance.
Equipment choices typically support foot grounding, postural alignment and safe weight‑bearing so that learners can plan and execute functional movements more effectively.
StandSure Therapy Aid is one example of a device presented as compatible with conductive education practice. It is described as providing a stable foot base to support sit‑to‑stand transitions, standing and kneeling while encouraging users to plan and perform each movement deliberately.
Where equipment is introduced, centres usually assess whether it complements task series and rhythmic intention, and whether it supports progression towards independence rather than substituting for skill development.
StandSure and similar tools are often used alongside vibration platforms, wobble boards, steps and standing frames already common in many centres; families should ask centres for evidence of compatibility and clinical reasoning for any device used.
StandSure Therapy Aid aligns with the key principles of conductive education by facilitating active participation in functional movement tasks. The stable foot base enables users to consciously plan and perform each movement within task series.
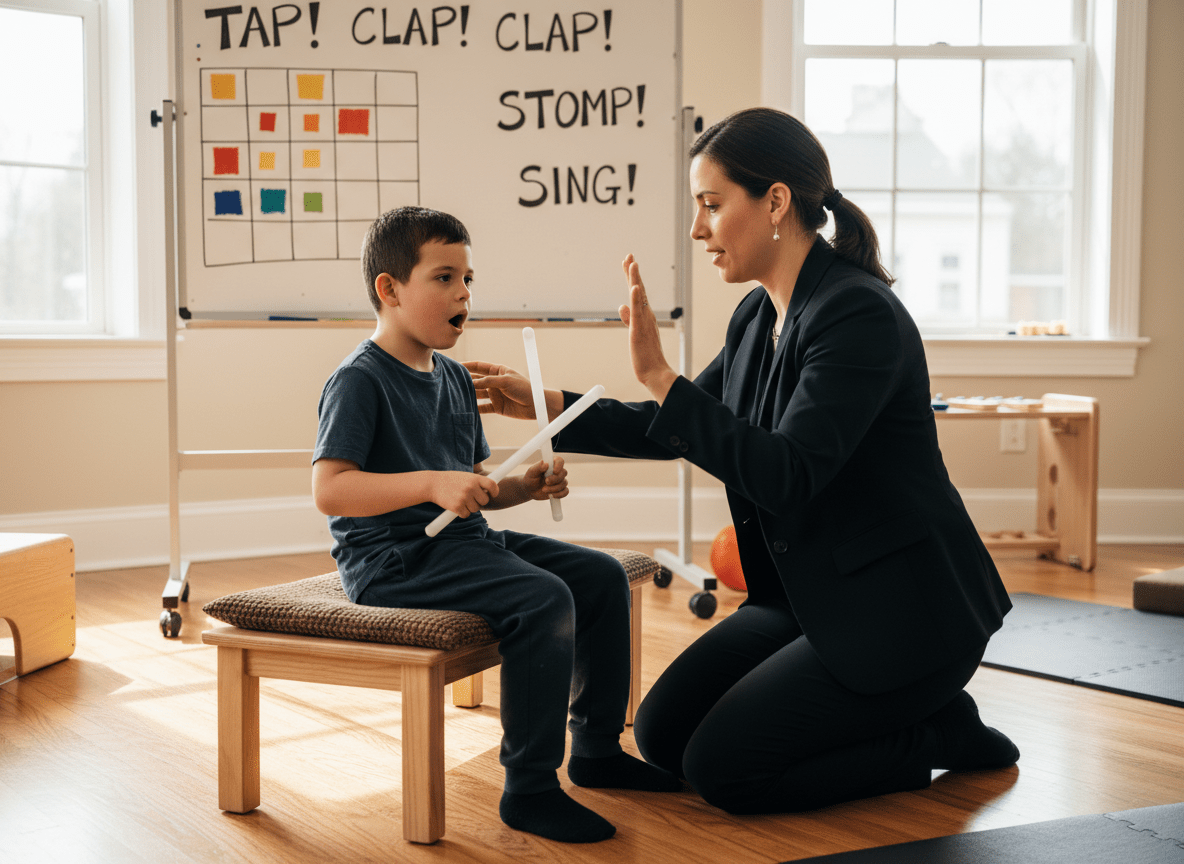
Rhythmic intention is a defining technique in conductive education. It involves speaking, chanting or singing short action‑based cues timed to movement, which links cognitive planning with motor execution.
The verbal rhythm provides temporal structure that aids sequencing of complex actions and helps maintain attention during repetition. In groups, shared vocal cues also support synchrony and motivation, reinforcing both motor and social learning.
The United Kingdom supports an established network of conductive education centres providing programmes across England, Scotland, Wales and Northern Ireland. Understanding how provision is organised helps families locate suitable services and plan access.
Conductive education in the UK expanded from small charitable initiatives in the late 1980s into a diverse sector serving many families. Centres vary in focus: some specialise in children with cerebral palsy, while others offer programmes for adults and people with a range of motor disorders.
Each centre adapts core conductive education principles to local needs and community contexts. Funding arrangements also differ: some centres operate as charities and rely on donations and fundraising, others charge fees or combine charitable support with family contributions, and a minority receive statutory support from local authorities or health services.
Geographic coverage is uneven. Urban areas and regions with strong advocacy networks commonly have better access to local provision, whereas families in more rural areas may need to travel or seek residential blocks to access intensive programmes.
Residential or block‑based options are offered by some centres to facilitate access for those who live at a distance. These models permit intensive intervention while reducing the need for long‑term daily travel.
Practical steps for families seeking provision include contacting local centres directly, checking available directories and parent networks, discussing potential statutory funding or support with local authorities, and asking centres about trial sessions, outreach options or block programmes that may suit particular needs and living circumstances.
Finding an appropriate conductive education centre is a key step for families considering this approach. The directory below lists established providers across the United Kingdom; contacting centres directly will help families assess suitability, programme intensity and practical arrangements.
Each centre adapts conductive education principles to local needs. When contacting a centre, consider asking about assessment procedures, programme formats (intensive blocks, weekly sessions or outreach), specialist equipment used and any available funding or support options.
Location: Essex
Supports children with disabilities through conductive education programmes tailored to individual needs. Offers early intervention and school‑age services focused on functional outcomes.
Location: Hampshire
Delivers comprehensive conductive education programmes alongside complementary therapies, with flexible session options to meet family needs.
Location: Herefordshire
Provides conductive education in a supportive setting for children with cerebral palsy and related conditions, emphasising family partnership and daily living skills.
Location: Aylesbury
Established provider offering conductive education from infancy through school age, including intensive blocks and ongoing support tailored to developmental goals.
Location: Sheffield
A specialist school combining standard curriculum with conductive education principles to support motor and academic development for school‑age children.
Location: London
London‑based centre providing conductive education for children with cerebral palsy, with a range of programme intensities to suit different family circumstances.
Location: London
The London Centre for Children with Cerebral Palsy offers early intervention and family‑centred conductive education programmes focused on movement learning.
Location: Bristol
Serves the South West with programmes for children and young people that emphasise functional skills and independence in everyday activities.
Location: Kent
Offers conductive education services in Kent aiming to promote independence and confidence for children with motor difficulties.
Location: Wirral
Merseyside charity providing conductive education for children with cerebral palsy, offering varied intensity levels and family support services.
Location: Darlington
North East centre delivering conductive education with an integrated educational approach for children across a range of abilities and ages.
Location: Nottingham
Midlands centre focusing on family partnership and achievement of functional goals in everyday situations.
Location: Leicestershire
Provides conductive education and therapy services for children with neurological and developmental conditions, with flexible programme structures.
Location: Birmingham
Birmingham‑based organisation serving children and adults with motor disorders, offering long‑established conductive education programmes.
Location: Devon
South West provider delivering conductive education for children, with a focus on movement learning through engaging, functional activities.
Location: Northern Ireland
Provides conductive education services across Northern Ireland with multiple programme formats to suit family circumstances.
This directory lists major established providers, but smaller community programmes and individual practitioners also operate in many areas. Families are advised to research local options, contact several centres to compare approaches and ask about assessment, funding and trial sessions to determine the best fit for their needs.
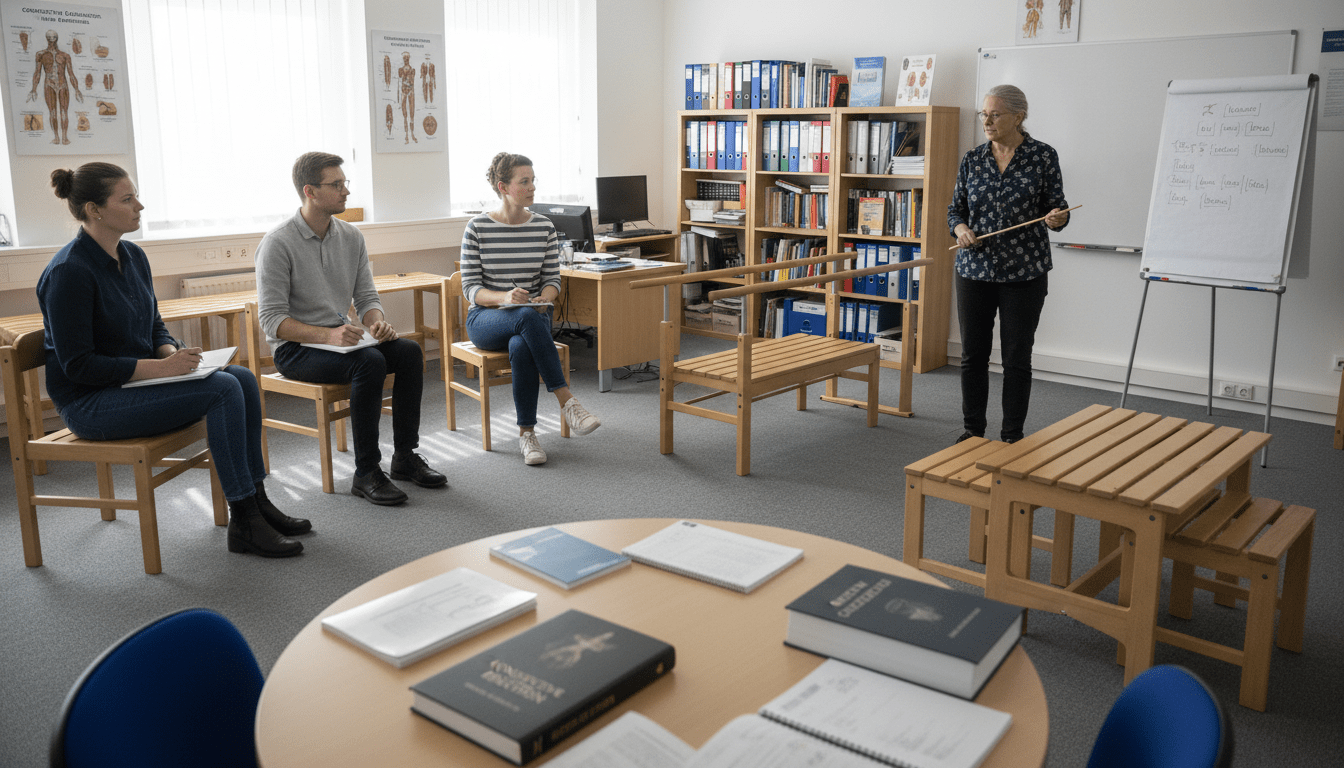
Preparation to work as a conductor combines pedagogical study with a practical understanding of motor disorders. Clarity about the training pathway helps families and professionals appreciate the expertise conductors bring to programme design and delivery.
Historically, conductor training was centred at the Pető Institute in Budapest; the original four‑year programme combined academic study with extensive clinical placements under experienced conductors.
UK training has developed more recently, increasing local access to qualifications. University and professional programmes now offer conductor education that includes theory, supervised clinical practice and assessment of competency in task series design and group facilitation.
The curriculum typically covers typical and atypical development, neurology, motor learning, pedagogy, psychology and practical methods for designing and delivering task series. Substantial placement experience ensures graduates can apply theoretical learning in real‑world settings.
Entry requirements vary between providers but commonly ask for prior qualifications or experience in education, therapy or healthcare. Mature applicants with relevant professional experience are frequently considered.
Programmes range from full‑time routes requiring several years of study to part‑time options for those already working in related fields. On completion, graduates receive formal recognition that qualifies them to work as conductors in conductive education centres; some institutions award academic degrees alongside professional qualification.
Professional learning continues after initial qualification. Conductors engage in continuing professional development to refine skills, remain current with practice developments and reflect on outcomes.
Many centres support ongoing learning through internal training, mentorship and apprenticeship models, where senior conductors guide less experienced colleagues. National and international conferences and peer networks provide additional opportunities for knowledge exchange and for discussing innovations in programme design and delivery.
Abstract principles are easier to understand through concrete examples. The examples below illustrate how task series and group learning translate into functional skill development for daily life.
A typical morning task series may target the sequence from lying to sitting to standing — a fundamental daily activity for many children and adults with motor disorders.
Sessions often begin with participants positioned on plinths. Using rhythmic intention, learners verbalise short, action‑focused cues such as: “I grasp the rail. I pull myself to the side. I swing my legs down.” These spoken cues support motor planning and provide timing for each component.
Each element of the sequence is practised separately until it can be performed reliably; components are then combined into a smooth, functional routine. Conductors provide minimal, graded facilitation and close supervision to promote safety while encouraging independent problem‑solving.
Walking task series progress from basic weight‑shift and balance activities to stepping and coordinated gait. Early stages emphasise safe standing, controlled weight transfer and alignment.
Groups may practise between parallel bars or along marked pathways, with rhythmic chanting timed to steps: “I lift my foot. I move it forward. I place it down. I shift my weight.” This verbal mediation helps learners plan each element and supports gradual automation of the pattern.
Safety is central: close facilitation, appropriate equipment and graded challenge ensure practise occurs within each person’s abilities. Progression rates vary; some individuals advance rapidly, while others need prolonged repetition at each stage.
Hand function task series address grasp, release and manipulation skills essential for dressing, eating and personal care. Sessions use real objects — buttons, zips, utensils — so learning has immediate functional relevance.
Tasks are practised in small, repeated steps and rehearsed within the group context. Peer observation and encouragement increase motivation and help generalise skills to home and school activities.

The group setting creates important learning advantages. Observing a peer successfully complete a task provides a clear model and tangible evidence of what is possible.
Turn‑taking teaches patience and sustained attention; while waiting, individuals often mentally rehearse the next action and offer verbal support. These processes reinforce both motor and communication skills.
Social relationships commonly develop from group participation. Children especially benefit from peer connections, which reduce isolation and often continue outside formal sessions. As with other outcomes, the pace and extent of social gains depend on individual temperament and programme consistency.
Families and professionals frequently ask whether conductive education is suitable for individuals on the autism spectrum. Clarifying the relationship between motor difficulties and autism, and the adaptations commonly used, supports informed decision‑making.
Many people with autism experience motor coordination challenges that affect daily functioning. Difficulties with planning and sequencing movement — often described as dyspraxia — can interfere with activities such as dressing, handwriting and play.
Sensory processing differences are also common and may affect proprioception or balance, adding complexity to movement planning and execution. These factors can compound challenges in independence and everyday tasks.
Conductive education was not originally developed specifically for autism, but its motor‑learning focus can benefit individuals who have significant movement difficulties. The structured, predictable format of task series and the emphasis on repetition and planning may suit those who respond well to routine and clear verbal or visual cues.
However, the group setting may be advantageous for some and overwhelming for others. Suitability depends on individual sensory preferences, social tolerance and the ability to engage with the learning process.
Centres working with children and adults on the autism spectrum commonly adapt standard programmes. Typical adaptations include:
Assessment by a qualified conductor, ideally undertaken in collaboration with occupational therapy and speech and language therapy when relevant, will determine whether conductive education forms an appropriate component of a wider intervention plan.
Alternative or complementary approaches may better address core social‑communication or sensory needs, while conductive education can specifically target motor learning where this is a priority.

Suitability depends on the nature of the child’s motor difficulties, cognitive profile and readiness for group learning. Conductive education is particularly appropriate for children whose primary challenges relate to movement and functional skills, such as those with cerebral palsy or spina bifida.
A formal assessment by a qualified conductor provides the most reliable guidance. Most centres offer an initial consultation to review goals, observe abilities and recommend a programme format.
Practical questions to raise at assessment include: What are the specific goals for the child? How will task series be adapted? What level of facilitation is planned and how will progress be measured?
Benefits commonly span motor, cognitive and social domains. Improvements often include better posture, balance and coordination, alongside enhanced functional skills for daily activities.
The integrated learning approach also supports planning, sequencing and problem‑solving skills that transfer to everyday situations. Group participation tends to foster communication, confidence and peer relationships.
Outcomes vary between individuals. Some children make rapid gains while others progress more gradually. Consistent participation, programme intensity and family involvement are important influences on results.
It is important to have realistic expectations: conductive education does not cure cerebral palsy or remove all motor difficulties, but it can help a child develop strategies to maximise independence and functioning within their abilities.
Session length varies by centre and programme type. Traditional intensive programmes often run for three to four hours daily, providing repeated practice across multiple task series.
Shorter options (one to two hours) are commonly offered for very young children or for families unable to commit to full‑day attendance. Block programmes deliver intensive full‑day sessions over consecutive weeks, often during school holidays.
Maintenance or follow‑up programmes may meet once or twice weekly for shorter periods to consolidate gains. The optimal schedule depends on individual goals, family capacity and the centre’s model of delivery.
When discussing options with a centre, ask about typical programme formats, expected intensity for desired outcomes and whether trial sessions or block placements are available.
Conductive education presents a distinctive, education‑centred approach to supporting people with motor disorders. By integrating learning, movement and personality development within a single system, the methodology addresses functional needs that segmented therapy models may not fully cover.
The approach requires active participation from learners. This requirement is a strength—those who engage consistently with task series and practice often achieve meaningful functional gains—but it is also an important consideration when assessing suitability.
There is an extensive but uneven network of centres across the United Kingdom offering programmes and access to qualified conductors. Some families find local provision; others choose block or residential options to access intensive programmes. Discussing local availability and funding with centres and statutory services will clarify practical options.
Modern practice sometimes incorporates complementary equipment and adjunct approaches that align with core principles. Any tool or device introduced should support active participation in functional movements and be integrated with clear therapeutic and educational goals.
Choosing a programme benefits from evidence‑based enquiry and dialogue: review centre information, arrange an initial assessment, speak with conductors about goals and methods, and consult healthcare professionals as needed. Connecting with other families can offer practical perspectives on day‑to‑day implications and likely outcomes.
The path through conductive education demands commitment from the learner, family and professionals working in partnership. For many, the reward is greater independence and improved quality of life; realistic, person‑centred goals and steady practice form the foundation for progress.
Book a personalised demonstration of the StandSure™ today by filling out our request form. Have any questions? Call us now, and our team will be happy to assist!



