No products in the cart.
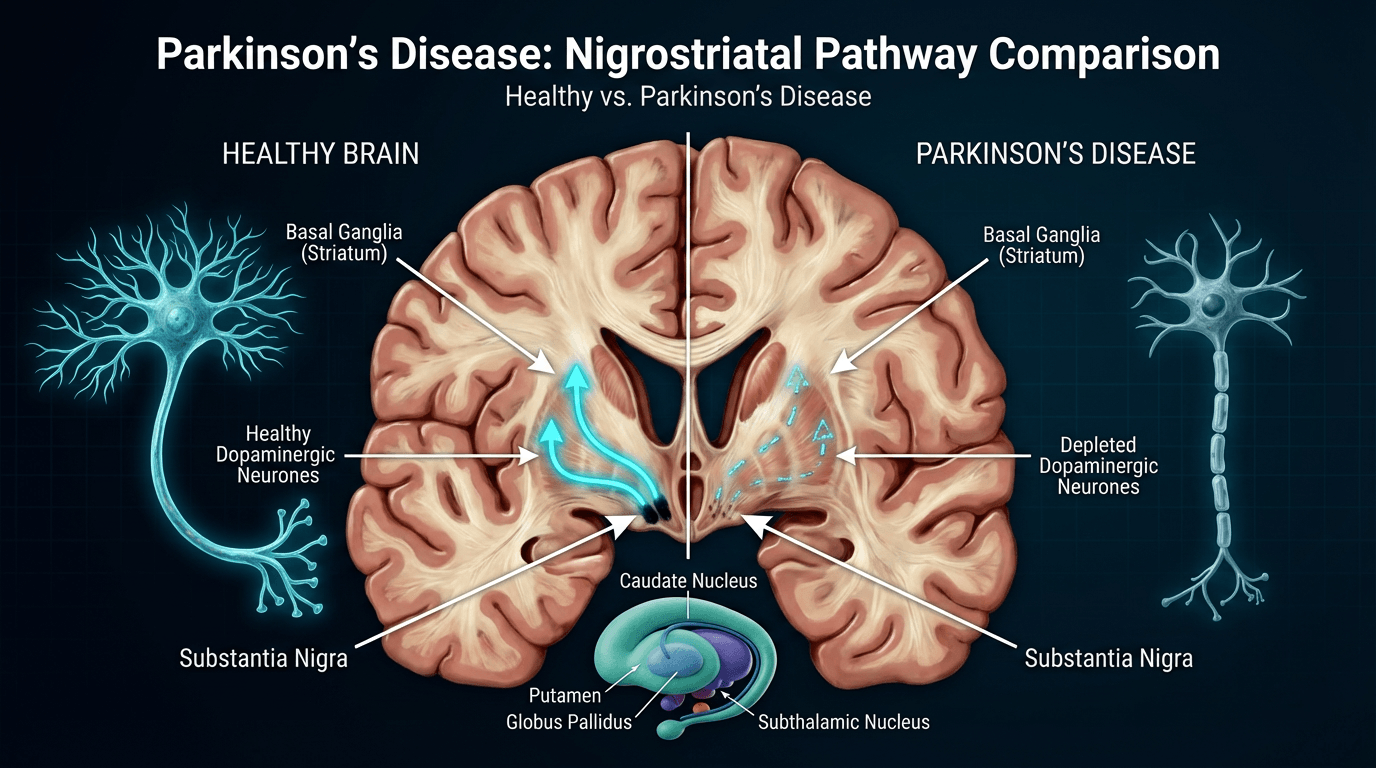
Parkinson’s disease is a progressive neurological condition that primarily affects the nervous system, targeting regions of the brain responsible for coordinating movement. The disorder develops as nerve cells in the substantia nigra — a deep brain structure involved in motor control — progressively deteriorate and are lost.
These specialised neurones produce dopamine, a chemical messenger essential for smooth, controlled movement. As dopamine levels fall, characteristic motor features become apparent and typically increase in severity over time.

In the United Kingdom the condition affects an estimated 145,000 people, with about 18,000 new diagnoses each year. Symptoms most commonly begin after age 60, although younger-onset cases occur in roughly 5–10% of individuals.
The pathological hallmark is the presence of Lewy bodies: intracellular deposits containing aggregated alpha-synuclein protein. These abnormal inclusions disrupt cellular function and contribute to neuronal death.
Loss of dopamine-producing neurones in the substantia nigra impairs the basal ganglia circuits that coordinate voluntary movement. The resulting neurochemical imbalance produces the typical movement difficulties seen in Parkinson’s disease.
The disorder is chronic and progressive rather than acute, and symptoms usually worsen gradually over months and years.
Clinical assessment distinguishes Parkinson’s disease from other movement disorders. For example, essential tremor typically occurs during action, whereas Parkinson’s tremor is most prominent at rest.
Conditions such as multiple system atrophy and progressive supranuclear palsy produce parkinsonian features but involve different brain regions, often progress more rapidly, and respond less well to dopaminergic therapies.
Accurate specialist assessment is essential to establish the correct diagnosis and to guide appropriate treatment and prognosis.
Early recognition of Parkinson’s disease supports timely clinical assessment and initiation of appropriate treatment. The condition presents with a variable combination of motor and non-motor symptoms; the precise pattern and timing differ between individuals.

The principal motor features are tremor, rigidity, bradykinesia and postural instability. These cardinal signs underpin the clinical diagnosis and commonly begin asymmetrically, affecting one side of the body more than the other.
Tremor is often the most recognisable sign and is present at onset in many cases. The typical resting tremor may start in one hand and can appear as a rhythmic “pill-rolling” movement between the thumb and forefinger; it usually lessens with voluntary movement and disappears during sleep.
Bradykinesia — slowness of movement — is seen as reduced arm swing when walking, diminished facial expression and difficulty initiating actions. Routine tasks may feel slower and require conscious effort.
Rigidity produces limb stiffness and resistance to passive movement. Over time this contributes to reduced range of motion, changes in posture and the characteristic shuffling gait seen in later stages.
Non-motor symptoms frequently precede motor features by several years and have a major effect on quality of life. Sleep disorders, including REM sleep behaviour disorder, may emerge a decade or more before motor signs in some people.
Loss of smell (anosmia) is a common early finding but is non-specific. Autonomic involvement leads to problems such as constipation, urinary dysfunction and excessive sweating.
Cognitive changes range from mild impairment to dementia and become more common in later stages. Mood disorders — depression, anxiety and apathy — affect a substantial proportion of patients and warrant active treatment.
Blood pressure instability, particularly orthostatic hypotension causing dizziness on standing, reflects autonomic dysfunction and requires careful management to reduce fall risk.
No single investigation confirms Parkinson’s disease. Diagnosis relies on a detailed medical history, focused neurological examination and observation of response to dopaminergic medication where appropriate.
DaTscan is a supportive investigation that identifies reduced dopamine transporter activity in the brain and can help distinguish Parkinson’s disease from essential tremor and some other mimics; access and interpretation should follow local specialist guidance.
Clinical diagnostic criteria require bradykinesia plus at least one of resting tremor, rigidity or postural instability. Specialist assessment by a neurologist or movement disorder service improves diagnostic accuracy, particularly in early or atypical presentations.
Subtle changes may precede classic motor symptoms. Micrographia (smaller, cramped handwriting), reduced voice volume and monotonous speech are common early indicators.
Facial masking — reduced spontaneous expression and decreased blinking — and slowed automatic movements are frequently overlooked by patients and families until more obvious signs develop.
REM sleep behaviour disorder (acting out dreams), chronic constipation, low mood and persistent fatigue are other early clues that should prompt clinical review.
Seeking Timely Assessment: Recognising early symptoms and obtaining specialist evaluation enables access to appropriate treatments and support. NHS routes commonly begin with GP referral to neurology; keeping a symptom diary documenting changes in movement, sleep and daily function can assist clinical assessment.
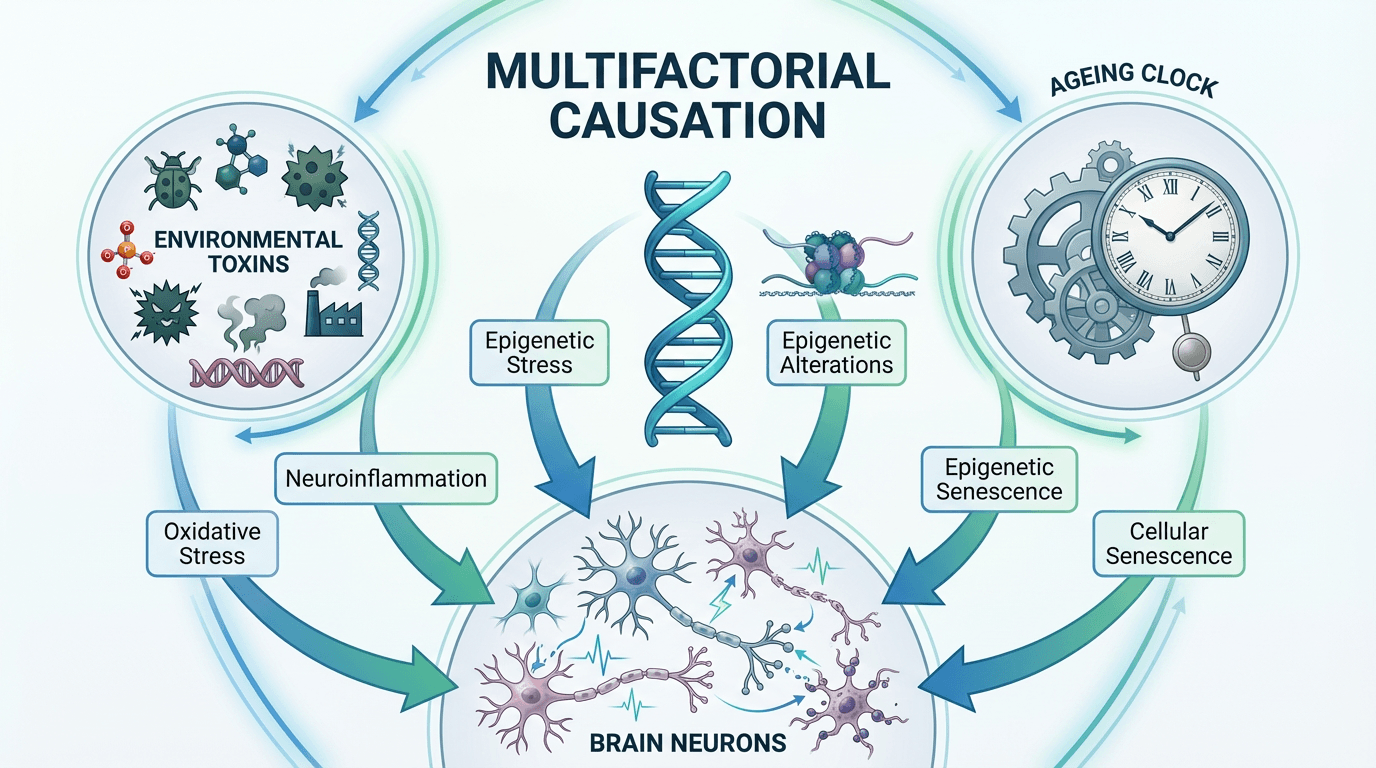
The exact triggers of dopamine-producing neuron loss in Parkinson’s disease remain incompletely understood. Evidence indicates a multifactorial origin in which genetic susceptibility interacts with environmental and lifestyle exposures to increase risk.
Approximately 10–15% of cases show clear familial patterns with identifiable mutations. Variants in genes such as LRRK2 and SNCA are linked to autosomal dominant forms, while Parkin, PINK1 and DJ-1 mutations are more often associated with younger-onset disease.
These genetic alterations affect cellular processes including mitochondrial function and protein degradation, increasing neuronal vulnerability. The GBA variant—associated with Gaucher’s disease—raises lifetime risk but does not inevitably cause Parkinson’s disease on its own.
Most cases remain sporadic, reflecting a complex genetic architecture in which multiple common variants contribute modest risk as revealed by genome-wide association studies.
Epidemiological studies have linked certain environmental exposures to increased risk. These include contact with some pesticides and industrial chemicals, rural agricultural exposures and occupational contact with heavy metals in specific industries.
Head trauma, particularly repeated injuries, appears to elevate the risk of later parkinsonism through inflammatory and degenerative mechanisms. Conversely, population studies consistently show lower Parkinson’s disease risk associated with regular physical activity and higher caffeine intake.
Mitochondrial dysfunction is a central pathological feature, with impaired cellular energy production rendering neurones more susceptible to injury. Oxidative stress and accumulation of damaged proteins further compromise cell viability.
Misfolding and aggregation of alpha-synuclein form Lewy bodies, intracellular inclusions that disrupt normal cell function and are a pathological hallmark of the disease. Failure of protein-clearance systems such as the ubiquitin–proteasome and autophagy pathways exacerbates toxic accumulation.
Chronic neuroinflammation, mediated by activated microglia and astrocytes, contributes to progressive neuronal loss once protective acute responses become maladaptive.
Advancing age is the strongest risk factor for Parkinson’s disease. Age-associated declines in antioxidant defence, protein clearance and cellular repair mechanisms leave dopamine-producing neurones particularly vulnerable.
Symptoms commonly emerge later in life because the brain compensates for gradual neuronal loss until a critical threshold of dopaminergic cell loss is reached. This cumulative process explains the typical onset in older adults.
Treatment for Parkinson’s disease aims to manage symptoms, preserve function and optimise quality of life rather than provide a cure. A multidisciplinary approach—combining pharmacological therapies, surgical options and rehabilitative support—delivers the best outcomes for most people.
Choice of medication depends on age, symptom severity, functional priorities and tolerance of side effects. In younger people, dopamine agonists are often used initially to delay levodopa and reduce the long-term risk of motor complications; older patients commonly start levodopa because of its superior symptomatic efficacy and lower risk of neuropsychiatric adverse effects.
Treatment is individualised and adjusted frequently as the disease evolves. Careful timing and dose titration aim to maximise “on” time and minimise motor fluctuations and treatment-related adverse effects.
Levodopa remains the most effective drug for controlling motor symptoms. It is a precursor of dopamine that is converted to the active neurotransmitter within remaining neurones.
Co-prescription with a peripheral dopa-decarboxylase inhibitor (carbidopa or benserazide) increases central delivery and reduces peripheral side effects. Immediate-release tablets typically provide several hours of benefit per dose; extended-release and dispersible preparations may be helpful for specific symptom patterns or swallowing difficulties.
After years of treatment some people develop motor complications such as wearing-off (return of symptoms as a dose effect wanes) and dyskinesias (involuntary movements). Management strategies include dose redistribution, adjunctive therapies and device-assisted options for advanced fluctuations.
Dopamine agonists (for example pramipexole, ropinirole and transdermal rotigotine) directly stimulate dopamine receptors and can be used as monotherapy in early disease or as levodopa-sparing adjuncts. They may delay the onset of levodopa-related motor complications in selected patients.
Common adverse effects include nausea and orthostatic hypotension; a subset of patients develop impulse control disorders (such as pathological gambling or compulsive buying), which require prompt recognition and medication review.
MAO‑B inhibitors (rasagiline, selegiline, safinamide) slow dopamine breakdown in the brain and may offer modest symptomatic benefit. COMT inhibitors (entacapone, opicapone) prolong levodopa action by blocking peripheral metabolism and are useful for reducing predictable wearing-off.
Both classes are commonly used as adjuncts to levodopa to extend “on” time; drug interactions and side-effect profiles should be considered when prescribing.
Anticholinergics (such as trihexyphenidyl) may benefit younger patients with prominent tremor but are generally avoided in older people because of cognitive and urinary side effects. Amantadine can reduce levodopa-induced dyskinesias and is available in immediate and extended-release formulations.
Treatment Optimisation: Regular specialist review is essential to keep medication regimens effective and safe. Parkinson’s disease nurse specialists provide practical medication advice, monitor symptom patterns and support adherence between consultant appointments.
Rehabilitation complements pharmacological treatment by targeting functional limitations, preserving independence and improving quality of life. Evidence-based therapies address specific symptom domains and adapt as needs change throughout the disease course.

Physiotherapy focuses on gait, balance and mobility through tailored exercise programmes. Regular physical activity maintains muscle strength, flexibility and cardiovascular fitness and may help reduce symptom burden.
Cueing techniques—visual, auditory or tactile—assist with freezing of gait by providing external prompts to initiate and maintain movement. Simple examples include floor markers, rhythmic music and metronome pacing.
Balance training and targeted postural exercises reduce fall risk and improve confidence. Approaches such as tai chi, adapted dance and specific balance protocols have demonstrated clinical benefit.
Amplitude-based therapies (for example LSVT BIG) teach exaggerated, large movements to counteract bradykinesia and often produce durable improvements in functional mobility.
Occupational therapists assess everyday tasks and introduce practical strategies to preserve independence. Interventions include adaptive equipment, energy conservation techniques and home modifications such as improved lighting and grab rails.
Fine motor training addresses difficulties with handwriting, dressing and meal preparation; compensatory strategies and assistive devices help maintain participation in meaningful activities.
Cognitive-rehabilitation techniques support planning, organisation and multitasking where executive dysfunction is present. These interventions aim to maintain activity and reduce carer burden.
Speech therapists treat reduced voice volume, poor articulation and swallowing problems. The Lee Silverman Voice Treatment (LSVT LOUD) is an evidence-based programme that improves vocal loudness and speech clarity.
Swallowing assessment identifies dysphagia and aspiration risk; dietary adjustments, swallowing exercises and postural strategies reduce choking incidents and help maintain adequate nutrition.
Communication aids—amplifiers, pacing techniques or communication boards—support social interaction and help prevent isolation.
Conductive Education combines physical, cognitive and social elements in structured group sessions and may benefit some people by promoting active learning and problem-solving for movement difficulties. Group delivery offers peer support and shared learning that can enhance motivation and wellbeing.
Regular aerobic exercise (walking, cycling, swimming) supports cardiovascular health and functional capacity. Resistance training maintains muscle mass and strength, while flexibility routines and yoga address rigidity and postural change.
Specialist classes—such as physiotherapist-led Parkinson’s boxing programmes—offer combined cardiovascular, coordination and balance training and are increasingly available in community settings.
Adjunctive therapies such as massage and music therapy may improve comfort, reduce muscle tension and support mood. Evidence for acupuncture is limited; realistic expectation-setting is important when considering complementary options.
Accessing Therapy Services: NHS physiotherapy, occupational therapy and speech and language therapy are available via GP or specialist referral. Parkinson’s-specific classes and local exercise groups are often provided by leisure services and charities; Parkinson’s UK maintains a directory of local opportunities and therapeutic services across the United Kingdom.
Medication management is the cornerstone of symptomatic treatment in Parkinson’s disease. Multiple drug classes target different aspects of dopaminergic dysfunction; understanding mechanisms, typical dosing and likely side effects supports informed treatment decisions and safer care.
Immediate-release levodopa combined with a peripheral dopa-decarboxylase inhibitor (co‑careldopa or co‑beneldopa) provides the most consistent motor benefit. Typical benefit from a single immediate‑release dose lasts several hours; dose and frequency are individualised according to symptom control and tolerance.
Controlled‑release and dispersible preparations offer alternative pharmacokinetic profiles useful for overnight control or for patients with swallowing difficulties. Continuous intestinal gel infusion delivers levodopa directly to the duodenum and is considered for selected patients with severe, treatment‑refractory motor fluctuations.
Dopamine agonists (for example pramipexole, ropinirole and transdermal rotigotine) stimulate dopamine receptors directly and may be used as initial monotherapy in younger patients or as adjuncts to levodopa. Extended‑release formulations permit once‑daily dosing and can improve adherence and symptom stability.
Common adverse effects include nausea and postural hypotension. A notable risk is the development of impulse control disorders (pathological gambling, compulsive shopping or hypersexuality); carers and clinicians should monitor behaviour and review therapy if concerns arise.
MAO‑B inhibitors (rasagiline, selegiline, safinamide) reduce central dopamine breakdown and provide modest symptomatic benefit, often as early monotherapy or as an adjunct to levodopa. COMT inhibitors (entacapone, opicapone) extend levodopa action by limiting peripheral metabolism and are useful for predictable wearing‑off.
Drug interactions are important—particularly with MAO‑B inhibitors—so prescribing should follow specialist guidance and medicines reconciliation.
Wearing‑off (symptoms returning before the next dose) can be managed by altering dose timing, adding adjunctive agents or using extended‑release preparations. Dyskinesias (involuntary movements associated with peak dopaminergic effect) may respond to levodopa dose redistribution or to amantadine, which reduces dyskinesia severity in many patients.
For unpredictable “on–off” phenomena, options include liquid levodopa formulations, apomorphine rescue therapy or device‑assisted therapies in appropriate candidates; specialist movement disorder teams guide these choices.
Non‑motor features frequently require pharmacological treatment. Depression often responds to selective serotonin reuptake inhibitors, bearing in mind potential interactions with MAO‑B inhibitors. Cognitive decline in Parkinson’s disease dementia may receive modest benefit from cholinesterase inhibitors such as rivastigmine.
Orthostatic hypotension can be managed initially with non‑pharmacological measures (increased fluids and salt, compression stockings); pharmacological options include fludrocortisone or midodrine when necessary. Sleep disorders, urinary symptoms and other autonomic issues also commonly require targeted treatment.
| Medication Class | Primary Mechanism | Common Examples | Typical Dosing | Key Considerations |
| Levodopa | Dopamine precursor | Co-careldopa, Co-beneldopa | 50-100mg 3-6 times daily | Most effective; motor complications may develop over time |
| Dopamine Agonists | Direct receptor stimulation | Pramipexole, Ropinirole, Rotigotine | Variable by agent | Impulse control disorder risk; nausea and hypotension common |
| MAO-B Inhibitors | Prevent dopamine breakdown | Rasagiline, Selegiline, Safinamide | Once daily | Drug interactions; modest symptomatic benefit |
| COMT Inhibitors | Extend levodopa duration | Entacapone, Opicapone | With each levodopa dose or once daily | Diarrhoea common; requires concurrent levodopa |
| Amantadine | NMDA antagonist | Amantadine immediate and extended-release | 100mg 2-3 times daily or once daily ER | Anti‑dyskinesia effect; monitor for cognitive effects and leg swelling |
Precise timing of medications is critical for symptom control. Levodopa absorption is affected by food; taking it 30–60 minutes before meals often improves efficacy, and spreading protein intake towards the evening may reduce daytime absorption interference.
Use of pill organisers, mobile reminders and involvement of carers can support adherence to complex regimens. Missing doses may precipitate worsening symptoms and, in some cases, unsafe mobility impairment.
Navigating complex medication regimens requires specialist input and regular review. Parkinson’s disease nurse specialists and movement disorder clinics provide medication counselling, dose optimisation and support for side‑effect management.
Surgical interventions can provide substantial symptomatic benefit for carefully selected people who continue to experience disabling motor complications despite optimised medications. Deep brain stimulation is the principal device-based option; alternative lesioning techniques may suit patients with specific symptom profiles or contraindications to implanted systems.
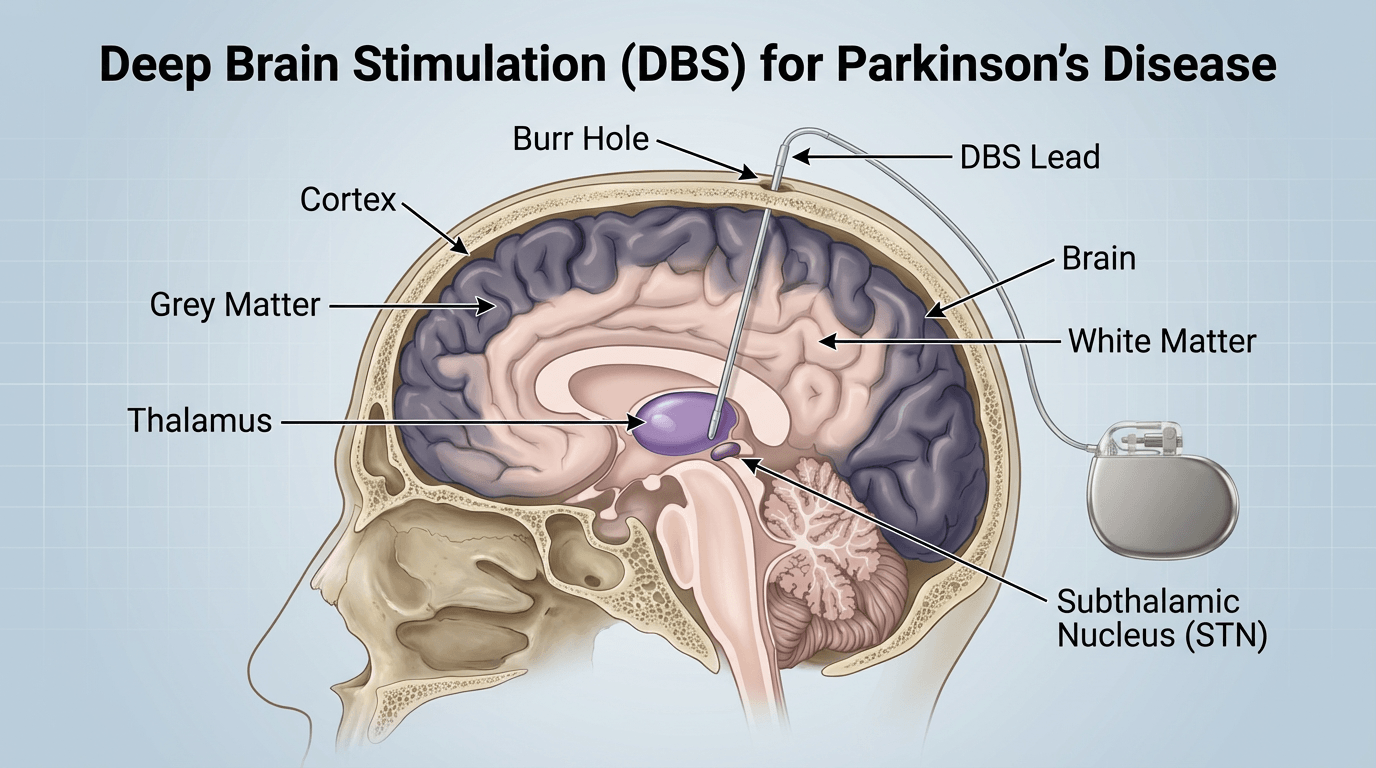
Deep brain stimulation (DBS) involves placement of electrodes into targeted deep brain structures—most commonly the subthalamic nucleus or the globus pallidus internus. High‑frequency electrical stimulation modulates abnormal neural activity within motor circuits and reduces core motor features.
The operation is typically performed in stages: electrode implantation with intraoperative neurological testing, followed by subcutaneous placement of the pulse generator under general anaesthesia. Leads are connected to a battery‑powered stimulator positioned beneath the clavicle.
Appropriate candidate selection is crucial. Ideal features include a robust response to levodopa, troublesome motor fluctuations or dyskinesias, absence of significant dementia or unstable psychiatric disease, and realistic expectations about achievable benefits. Age alone is not an absolute exclusion, but overall medical fitness influences candidacy.
Most patients receive bilateral stimulation to address symptoms on both sides; unilateral procedures may be considered where symptoms remain strongly asymmetric.
DBS commonly produces marked improvement in tremor, rigidity and bradykinesia in the off‑medication state and reduces dyskinesias by permitting lower dopaminergic doses. Many patients experience increased daily “on” time without troublesome involuntary movements and an associated improvement in quality of life.
Medication requirements frequently fall after DBS—often by 30–50%—although most people continue to require some dopaminergic therapy. Modern systems provide durable benefit for many years, with battery replacement intervals varying by device type and usage.
Serious operative risks are uncommon but important. Intracranial haemorrhage occurs in a small proportion of cases and can, rarely, cause permanent neurological deficit. Device‑related infection may require antibiotics and sometimes hardware removal.
Stimulation can produce side effects such as speech disturbance, gait or balance changes, and mood alterations; these are often reversible with programming adjustments. Careful preoperative neuropsychological assessment helps identify individuals at higher risk of cognitive decline following subthalamic stimulation.
Lesioning procedures (pallidotomy, thalamotomy) create permanent focal interruptions in pathological circuitry and remain options where DBS is unsuitable. Focused ultrasound offers a non‑invasive, MRI‑guided unilateral thalamotomy for medication‑resistant tremor without implanted hardware. Stereotactic radiosurgery (Gamma Knife) can also generate targeted lesions in selected cases.
Initial programming typically begins several weeks after surgery to allow tissue recovery. Multiple follow‑up sessions optimise stimulation parameters (amplitude, pulse width, frequency) and guide concurrent medication reductions to achieve the best combined effect.
Ongoing specialist follow‑up is important to monitor device function, manage side effects and arrange battery replacement or recharge support. Remote programming is increasingly available in some services, reducing the need for frequent clinic visits.
Parkinson’s disease is clinically heterogeneous; recognising subtypes based on dominant features and progression patterns assists prognosis estimation and individualised treatment planning.
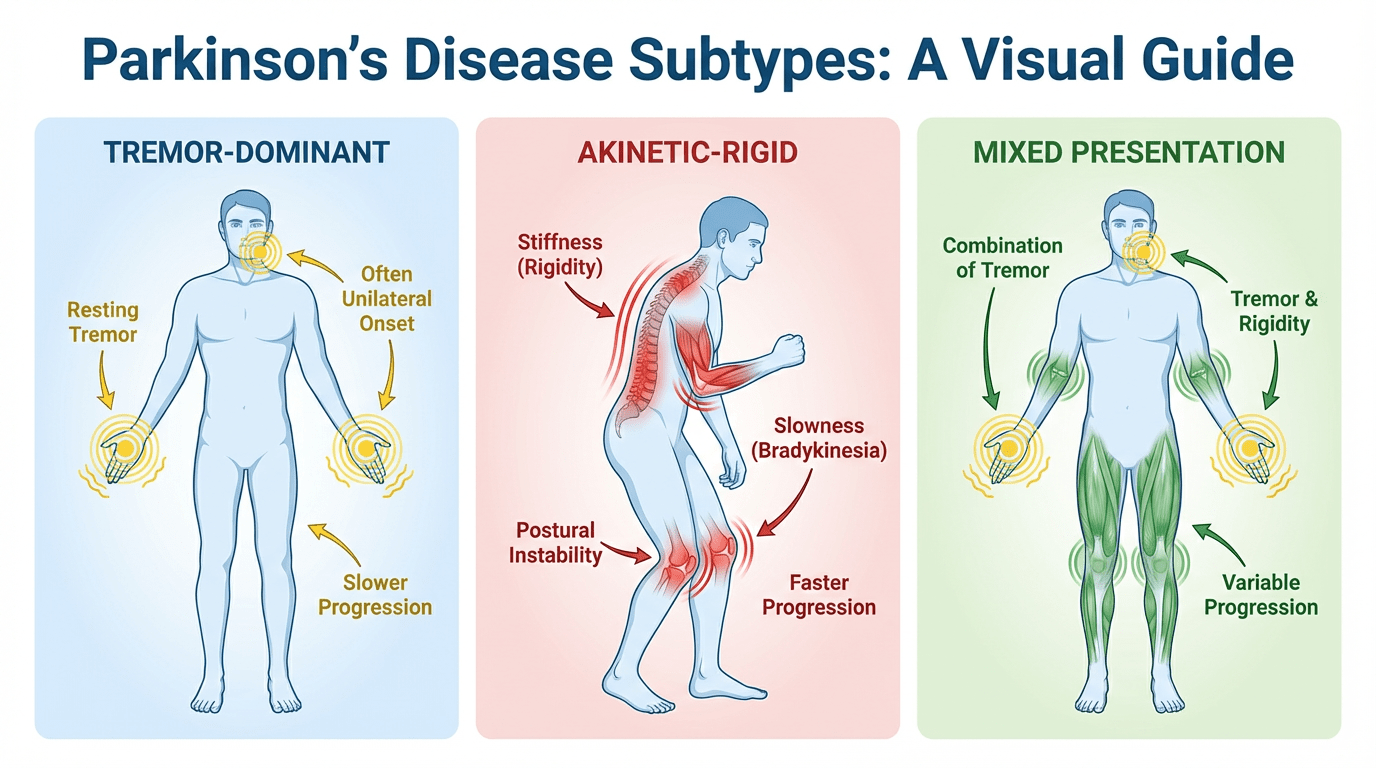
Tremor‑dominant presentations feature a prominent resting tremor and are often associated with slower progression and relatively preserved cognition. These patients frequently retain independence for longer and respond well to standard treatments.
The postural instability and gait difficulty (PIGD) subtype is characterised by balance problems, falls and freezing of gait. This pattern usually carries a higher risk of earlier disability and greater cognitive decline.
Akinetic‑rigid presentations show predominant bradykinesia and rigidity with minimal tremor; progression and cognitive risk tend to be intermediate between tremor‑dominant and PIGD forms. Mixed phenotypes are common and symptom profiles can evolve over time.
Young‑onset Parkinson’s disease, with symptom onset before age 50, accounts for a minority of cases. Genetic factors are more frequently implicated in this group. Although progression may be slower and levodopa responsiveness preserved, motor complications such as dyskinesias often appear earlier because of longer treatment exposure.
Psychosocial impacts — including effects on employment, finances and family planning — are particularly important in younger people and merit timely specialist support and practical advice.
Several distinct neurodegenerative conditions can present with parkinsonian features but differ in prognosis and treatment response. Multiple system atrophy combines parkinsonism with marked autonomic failure and cerebellar or pyramidal signs and typically shows poor levodopa response.
Progressive supranuclear palsy features vertical gaze impairment, early falls and frontal cognitive changes; clinical course is often more rapid than in typical Parkinson’s disease. Corticobasal degeneration presents with asymmetric rigidity, apraxia and cortical sensory loss and usually progresses quickly with limited therapeutic response.
Lewy body dementia shares pathology with Parkinson’s disease but is distinguished by early cognitive decline, prominent visual hallucinations and fluctuating cognition; motor features may be less marked or appear later.
Some genetic variants produce clinical syndromes similar to sporadic Parkinson’s disease. LRRK2‑related disease often resembles typical Parkinson’s disease with generally good treatment response. Autosomal recessive mutations (Parkin, PINK1, DJ‑1) more commonly underlie young‑onset parkinsonism and tend to show slower progression with sustained levodopa responsiveness.
GBA variants increase the risk of Parkinson’s disease and are associated with a higher likelihood of cognitive impairment in some patients.
Progression of Parkinson’s disease commonly follows recognised patterns, although timing and severity vary substantially between individuals. Staging systems assist clinicians to assess severity, guide management and communicate prognosis in clinical practice.
Stage 1 denotes unilateral motor involvement with minimal functional impairment. Symptoms at this stage—such as tremor or mild rigidity affecting a single limb—often have little effect on daily activities and may go unrecognised.
Stage 2 involves bilateral motor signs without balance impairment. Daily tasks may require more time or effort, but independence is typically maintained and many people continue working.
Stage 3 marks the onset of postural instability while independence is generally retained. Balance difficulties and occasional falls are common and this stage represents a pivotal point for intensified rehabilitation and fall prevention strategies.
Stage 4 reflects severe motor disability with preserved ability to stand or walk unaided only with difficulty. Activities of daily living usually require substantial assistance and independent living becomes challenging.
Stage 5 describes advanced disease with wheelchair or bed dependence. Complete assistance is required for most personal care needs and round‑the‑clock support is commonly necessary.
Modified Hoehn and Yahr grades (for example 1.5, 2.5) provide finer discrimination between the classical stages. Importantly, medication effects mean that function may differ between “on” and “off” states, so assessment should consider both when possible.
Rates of progression are highly individual. Some people remain in early stages for many years while others advance more rapidly; staging should therefore inform, but not determine, personal care planning.
The Unified Parkinson’s Disease Rating Scale (UPDRS), and its MDS‑UPDRS revision, offer comprehensive evaluation across motor and non‑motor domains. Part I addresses non‑motor experiences of daily living, Part II captures patient‑reported motor experiences, Part III comprises the clinician’s motor examination and Part IV documents motor complications such as dyskinesias and fluctuations.
Use of UPDRS/MDS‑UPDRS supports reproducible monitoring of disease trajectory and the impact of interventions over time.
Early disease often progresses slowly over the first five to ten years after diagnosis. Motor symptoms generally worsen gradually, necessitating adjustments in medication and therapy.
Mid‑stage disease typically brings motor complications such as wearing‑off and dyskinesias; functional independence may decline despite treatment optimisation. This stage commonly requires closer multidisciplinary input and rehabilitation to preserve activities of daily living.
Advanced disease is characterised by medication‑resistant symptoms, increased disability and frequent falls. Non‑motor features—particularly cognitive impairment and autonomic dysfunction—become more prominent and substantially affect quality of life.
End‑stage disease often requires comprehensive care, with complications such as dysphagia, recurrent infections and immobility contributing to complex medical needs and palliative care considerations.
| Stage | Motor Symptoms | Functional Impact | Typical Duration | Treatment Approach |
| Stage 1 | Unilateral tremor, rigidity or bradykinesia | Minimal disability; independence retained | Variable; often years | Monotherapy, exercise and lifestyle measures |
| Stage 2 | Bilateral symptoms, no balance impairment | Mild disability; independence maintained | Years to decade | Medication optimisation, therapy support |
| Stage 3 | Postural instability emerges | Moderate disability; some assistance required | Months to years | Combined therapy, fall prevention and rehabilitation |
| Stage 4 | Severe motor impairment | Significant disability; substantial assistance required | Variable progression | Complex regimens; consider DBS and enhanced support |
| Stage 5 | Unable to stand or walk unaided | Complete dependency | Months to years | Palliative focus; prioritise quality of life |
Cognitive decline commonly parallels motor progression: mild cognitive impairment may appear in mid stages and dementia develops in a substantial proportion over time. Autonomic dysfunction worsens, producing blood pressure instability, urinary symptoms and gastrointestinal problems that increase disability.
Psychiatric symptoms such as depression, anxiety, apathy and psychosis may fluctuate through the disease course and should be addressed proactively as part of holistic care.
Multiple factors influence susceptibility to Parkinson’s disease. Some exposures and characteristics increase risk while others show protective associations; understanding these elements helps identify at‑risk groups and informs clinical counselling without implying certainty of disease development.
Advancing age is the strongest risk factor: incidence rises markedly after 60 years. Although Parkinson’s disease can present at any age, median onset is in later life.
Male sex is associated with an increased risk compared with females; the reasons are likely multifactorial, including biological and exposure differences. Observed variations by ethnicity may reflect genetic, environmental or ascertainment factors.
Family history raises risk in first‑degree relatives and reflects shared genetic susceptibility and, at times, shared environmental exposures. A minority of cases (around 10–15%) have identifiable single‑gene causes or strong familial patterns.
Specific gene variants influence risk: LRRK2 and SNCA variants are linked to autosomal dominant forms, while Parkin, PINK1 and DJ‑1 mutations are more often associated with young‑onset parkinsonism. GBA variants increase lifetime risk but do not inevitably cause disease.
Large genome‑wide association studies have identified numerous loci each contributing small effects; cumulatively these common variants meaningfully affect susceptibility.
Epidemiological evidence links certain environmental exposures with increased Parkinson’s disease risk. These include contact with some pesticides and agricultural chemicals, rural agricultural work and occupational exposure to heavy metals or industrial solvents in particular settings.
Repeated head trauma is associated with greater risk of later parkinsonism, likely through chronic inflammatory and degenerative mechanisms. Risk relationships are generally dose‑related, with greater or repeated exposures conferring higher estimated risk.
Population studies consistently report inverse associations for certain exposures. Regular caffeine consumption and sustained physical activity are associated with lower Parkinson’s disease risk in many cohorts. Tobacco smoking also shows a paradoxical inverse association, although smoking carries substantial overall harms and is not a recommended preventive strategy.
Higher serum urate has been linked to reduced risk in observational studies, but cause–effect relationships remain unproven and are not a basis for clinical recommendations.
Some drugs can produce reversible drug‑induced parkinsonism (for example antipsychotics and metoclopramide) which typically improves after cessation. Evidence regarding medications that modify long‑term Parkinson’s disease risk is inconsistent; observational signals for agents such as statins warrant further investigation but do not establish causation.
Where possible, clinicians should advise on measures that reduce exposure and promote brain health.
These factors help identify individuals at higher baseline risk and inform surveillance or research approaches.
Certain jobs carry higher exposure risk and warrant occupational health measures.
These associations from population studies support public health advice promoting general brain health.
As Parkinson’s disease advances, a range of complications commonly arises that affect function, safety and quality of life. Many problems require specific management strategies in addition to standard dopaminergic therapies and benefit from coordinated multidisciplinary care.
Dyskinesias are involuntary, often choreiform movements that frequently develop after several years of levodopa treatment and are usually related to peak medication effect. Adjusting levodopa dosing strategies, increasing dose frequency or adding agents such as amantadine are typical management options.
Motor fluctuations—wearing‑off and on‑off phenomena—disrupt daily function. Wearing‑off describes the predictable return of symptoms as a dose effect wanes; on‑off fluctuations involve more unpredictable switches between good and poor mobility. Medication diaries help detect patterns and guide adjustments.
Freezing of gait is characterised by a sudden inability to start or continue walking, especially when turning or approaching doorways, and substantially increases fall risk. Physiotherapy, cueing techniques and medication optimisation form the mainstays of management.
Falls become more frequent as postural instability progresses. Contributing factors include motor impairment, orthostatic hypotension, visual problems and environmental hazards. Multidisciplinary fall prevention strategies are essential to reduce injury risk.
Mild cognitive impairment affecting executive function, attention and visuospatial skills is common; a substantial proportion of people show cognitive changes without dementia at diagnosis. Cognitive decline may progress to Parkinson’s disease dementia in later stages.
Neuropsychiatric problems are frequent. Depression affects many people and responds to pharmacological and psychological treatments. Anxiety and apathy are also common and warrant active management.
Visual hallucinations and psychosis most often occur in advanced disease or as medication effects; management typically begins with review and reduction of offending drugs and may include use of specialist antipsychotic treatment when necessary.
Impulse control disorders (pathological gambling, compulsive shopping, hypersexuality and binge eating) occur particularly in people receiving dopamine agonists. Early recognition and medication review are crucial.
Autonomic involvement produces a variety of troublesome symptoms. Orthostatic hypotension—failure to maintain blood pressure on standing—causes dizziness and increases fall risk; first‑line measures include increased fluid and salt intake, compression stockings and slow postural changes, with pharmacological options reserved for persistent cases.
Urinary problems (urgency, frequency, nocturia) and constipation are common and often predate motor features; simple measures such as hydration, dietary fibre and exercise help, with medications used when required.
Excessive sweating and skin conditions such as seborrhoeic dermatitis also occur and may worsen during off‑periods; symptom‑directed treatments improve comfort.
Sleep problems affect many people with Parkinson’s disease. Insomnia arises from motor symptoms, nocturia, medication effects and primary sleep disorders. Sleep hygiene measures and review of medication timing can improve sleep.
REM sleep behaviour disorder—acting out dreams due to loss of normal REM atonia—may precede motor symptoms and increases risk of bed‑partner injury; melatonin or clonazepam reduce episode frequency in many cases.
Excessive daytime sleepiness relates to nocturnal disturbance, medication effects (notably dopamine agonists) and disease‑related changes; it may impair daytime function and increase accident risk and therefore requires assessment.
Hypophonic dysarthria presents as reduced voice volume and unclear articulation; speech and language therapy, particularly LSVT LOUD, significantly improves vocal loudness and intelligibility for many people.
Dysphagia develops in a large proportion of patients over the disease course and carries aspiration risk, which contributes to pneumonia incidence. Early swallowing assessment and interventions (swallowing exercises, dietary texture modification, postural measures) reduce complications; urgent review is required for recurrent choking, unexplained weight loss or cough during eating.
Sialorrhoea (drooling) results from reduced spontaneous swallowing rather than excess saliva production and can be treated with behavioural strategies, anticholinergic medication, botulinum toxin injections to salivary glands or, rarely, radiotherapy in refractory cases.
Musculoskeletal pain, often related to rigidity, abnormal posture and reduced mobility, affects many people and may respond to physiotherapy, analgesia and postural correction. Dystonic pain can occur during off‑periods and may require targeted adjustment of dopaminergic therapy.
Central neuropathic pain reflects altered pain processing and may be poorly localised and resistant to standard analgesics; optimisation of Parkinson’s medications and specialist pain management approaches can help.
Radicular pain from spinal pathology is common and often benefits from physiotherapy and appropriate analgesia.
Comprehensive Complication Management: The multisystem nature of Parkinson’s disease complications requires coordinated multidisciplinary care. Regular specialist review enables early identification and timely intervention. Rapid clinical review is advised for red‑flag features such as recurrent aspiration, sudden changes in cognition or safety concerns following falls. Carers and family members should be included in planning and supported with information and respite options.
Parkinson’s disease meets the legal definition of disability under the Equality Act 2010 when symptoms substantially and adversely affect daily activities. This status provides important protections and access to a range of support services across the United Kingdom.

The Equality Act 2010 protects people with Parkinson’s disease from discrimination in employment, education and access to goods or services. Employers are required to consider and implement reasonable adjustments where these enable a person to carry out their role safely and effectively—for example flexible hours, adjusted duties or workplace adaptations.
Protection can apply from the point of diagnosis and does not require demonstration of current severe disability; this reflects the progressive nature of the condition and helps prevent unjust treatment based on future risk.
Direct discrimination—less favourable treatment because of the condition—and indirect discrimination—policies that disadvantage those with Parkinson’s without justification—are both unlawful. Employers should pursue open dialogue and occupational health advice to identify appropriate adjustments before considering dismissal.
Several statutory benefits may provide financial assistance. Personal Independence Payment (PIP) supports people with difficulties in daily living and mobility; assessments consider variability of symptoms and needs for prompting, supervision or physical help.
Other relevant benefits include Employment and Support Allowance for those unable to work and Attendance Allowance for people over state pension age who require regular care or supervision.
Practical advice from specialist advisers (for example Parkinson’s UK or local welfare rights services) is valuable when starting claims, preparing evidence and managing reassessments.
The Blue Badge scheme facilitates parking close to services for people with significant walking difficulties. Higher rate mobility PIP recipients are automatically eligible; discretionary awards may be issued by local authorities for others with substantial mobility impairment.
Badges permit parking in designated disabled bays and limited relaxations of on‑street restrictions, improving access to healthcare and community services.
Reasonable adjustments at work support continued employment. Examples include flexible start and finish times to accommodate medication schedules, adjusted duties to match changing capabilities, assistive technologies (voice activation, ergonomic keyboards) and phased return to work after illness.
Access to Work funding can help employers obtain specialised equipment or make workplace modifications where needed.
Local authority social care assessments determine eligibility for funded support. Assessments evaluate needs across personal care, domestic tasks and social participation, and result in a care and support plan identifying services such as personal care, domestic help, meal provision or respite for family carers.
Means testing may affect contributions toward cost of care; direct payments allow people to commission personalised support when eligible and appropriate.
Occupational therapy can recommend specialist equipment—adapted cutlery, dressing aids, bathroom adaptations and mobility aids—that preserves independence. Disabled Facilities Grants may help fund major home adaptations such as stairlifts or level‑access showers.
Technology solutions (medication reminders, fall detectors, telecare) support safety for people living alone and reduce carer anxiety.
Financial support for daily living and mobility needs. Two components are assessed separately based on functional impact; assessments consider fluctuating symptoms and “good” and “bad” days.
Provides financial support for people over state pension age who require frequent assistance or supervision due to disability.
Parking concessions to improve access for people with significant mobility limitations.
Extensive support networks across the United Kingdom offer practical help, information and community connection for people living with Parkinson’s disease and their families. Charitable organisations provide local services, specialist advice and fund research into improved treatments.
Parkinson’s UK is the principal UK charity offering comprehensive support. Services include evidence‑based information, local support groups, specialist advisers and funding for research that improves treatments and care.
More than 350 local groups operate throughout England, Wales, Scotland and Northern Ireland, providing peer support, condition‑specific exercise classes and educational events. These groups help people remain active and connected within their communities.
The confidential Parkinson’s UK helpline is staffed by trained advisers who can assist with symptom management queries, benefits advice and signposting to local services.
Access expert support, specialist information and links to local services across the UK. The Parkinson’s UK helpline provides confidential assistance for any questions or concerns.
Coordinates nationwide services and support across England.
Address: Parkinson’s UK, 50 Broadway, London SW1H 0DB
Phone: 020 7931 8080
Email: [email protected]
Charity Numbers: 258197 (England & Wales), SC037554 (Scotland)
Provides Scottish services and local support.
Address: Suite 1/10b, King James VI Business Centre, Riverview Business Park, Friarton Road, Perth PH2 8DY
Phone: 0344 225 3724
Email: [email protected]
Supports the Parkinson’s community in Northern Ireland.
Address: Wellington Park Business Centre, 3 Wellington Park, Malone Road, Belfast BT9 6DJ
Phone: 028 9092 3370
Email: [email protected]
Offers services in Welsh and English across Wales.
Address: Maritime Offices, Woodland Terrace, Maesycoed, Pontypridd CF37 1DZ
Phone: 0344 225 3784
Email: [email protected]
Cure Parkinson’s is a research charity focused on developing disease‑modifying therapies. The organisation funds clinical trials and experimental projects aimed at slowing, stopping or reversing the disease process.
Collaborations with academic centres and industry accelerate development of novel approaches such as drug repurposing, gene therapy and immunotherapy. While Cure Parkinson’s does not provide direct patient services, its research investment offers hope for future treatments.
Address: The Cure Parkinson’s Trust, 120 New Cavendish Street, London W1W 6XX
Phone: 020 7487 3892
Email: [email protected]
Website: cureparkinsons.org.uk
Charity Numbers: 1111816 (England & Wales), SC044368 (Scotland)

Other organisations provide complementary resources: the Parkinson’s Foundation offers extensive educational materials and research updates (useful online resources for UK audiences), Age UK supplies general support for older people, and Carers UK provides guidance and support for family carers.
Local authority adult social services arrange social care assessments and help access funded support packages when needs increase.
Accessing Local Support: Local Parkinson’s UK groups provide face‑to‑face connection, condition‑specific exercise classes and education. Contact the Parkinson’s UK helpline or visit their website to find local groups and services that match individual needs.
Short answer: diagnosis leads to education, a personalised management plan and access to treatment and support services.
Detailed explanation: after diagnosis a neurologist or specialist team explains the condition, expected course and treatment options and develops an individualised plan based on symptoms and function. Treatment may start immediately or be deferred for mild symptoms. Referrals to physiotherapy, occupational therapy and speech and language therapy are common. Early contact with support organisations, such as Parkinson’s UK (helpline 0808 800 0303), helps with practical advice and local services.
Short answer: loss of dopamine‑producing neurones in the substantia nigra, from a combination of genetic and environmental factors.
Detailed explanation: Parkinson’s disease results from progressive degeneration of dopamine‑producing cells in the substantia nigra, leading to disrupted basal ganglia function and characteristic movement disorders. The precise triggers are not fully understood; current evidence implicates a complex interplay of genetic susceptibility (including recognised mutations) and environmental exposures, together with cellular mechanisms such as mitochondrial dysfunction, oxidative stress, protein misfolding and neuroinflammation. Age is the strongest risk factor.
Short answer: a comprehensive, multidisciplinary approach tailored to individual needs.
Detailed explanation: optimal management combines pharmacological treatment (levodopa, dopamine agonists, MAO‑B inhibitors and adjuncts) with therapy input—physiotherapy, occupational therapy and speech and language therapy—and regular specialist review. Regular exercise, attention to non‑motor symptoms (sleep, mood, autonomic dysfunction) and involvement of Parkinson’s disease nurse specialists improve outcomes. Engagement with local support groups and services further enhances coping and quality of life.
Short answer: most cases are sporadic, but a minority have identifiable genetic causes or increased genetic risk.
Detailed explanation: about 10–15% of cases show clear familial patterns or single‑gene causes. Specific genes (for example LRRK2, SNCA, Parkin, PINK1, DJ‑1) are implicated in some families; GBA variants increase lifetime risk in a subset of people. However, most people with genetic risk variants never develop Parkinson’s disease, and a family history increases risk but is not determinative. Genetic counselling may be offered where relevant.
Parkinson’s disease presents ongoing challenges for movement, function and everyday wellbeing. Understanding the underlying mechanisms, recognising symptoms early and accessing coordinated treatment and support help people maintain independence and quality of life for many years following diagnosis.
Therapeutic options continue to expand. Improved medication formulations, refined rehabilitative therapies and advanced surgical interventions such as deep brain stimulation provide increasingly effective symptom control. Research supported by organisations including Cure Parkinson’s seeks disease‑modifying treatments and advances in clinical trials, offering hope for future progress.
Non‑pharmacological therapies—physiotherapy, occupational therapy and speech and language therapy—play a central role in preserving function. Innovative approaches, including Conductive Education, and regular physical activity support mobility, communication and participation in valued activities.
A well‑established support network across the United Kingdom provides practical assistance and community connection. Parkinson’s UK offers specialist advice, local groups and signposting to services; regional offices in Scotland, Wales and Northern Ireland deliver locally tailored support.
Living well with Parkinson’s disease requires comprehensive care addressing physical, cognitive, emotional and social needs. Multidisciplinary teams coordinate treatments and support, and involvement of family and community resources sustains long‑term wellbeing. With appropriate care and support, many people continue to pursue meaningful activities and maintain fulfilling relationships.
For those newly diagnosed, supporting a loved one or managing symptom change, expert help is readily available. Contacting specialist services or the Parkinson’s UK helpline provides personalised guidance and direct links to local resources and therapy options.
Whether facing a new diagnosis, experiencing changing symptoms, or supporting someone with Parkinson’s disease, specialist advisers can offer practical guidance, information and connection to local services across England, Wales, Scotland and Northern Ireland.
The journey with Parkinson’s disease can be demanding, yet many people across the United Kingdom lead fulfilling, meaningful lives despite neurological changes. With timely specialist care, tailored therapies and strong support networks, individuals can adapt, manage challenges and retain dignity throughout their experience.
Book a personalised demonstration of the StandSure™ today by filling out our request form. Have any questions? Call us now, and our team will be happy to assist!



