No products in the cart.
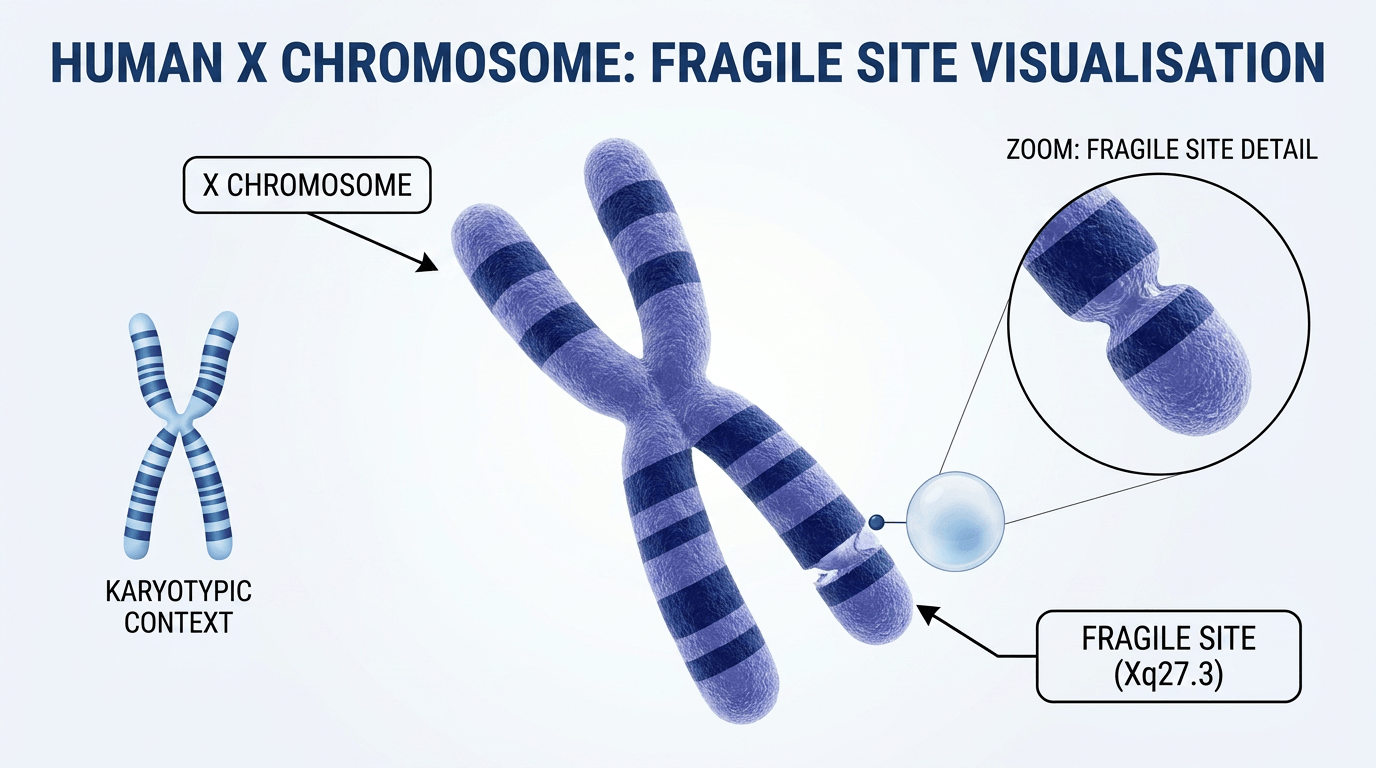
The FMR1 gene on the X chromosome directs production of a protein essential for early brain development. Excessive repetition of a short DNA sequence within this gene reduces or abolishes protein production, producing the biological basis of fragile X syndrome.
Laboratory testing measures the number of CGG repeats in the FMR1 gene. Typical laboratories report ranges as follows: 5–44 repeats (normal), 45–54 (intermediate), 55–200 (premutation) and over 200 (full mutation). A full mutation usually silences the gene and causes the clinical features of fragile x syndrome, while a premutation carries different health implications for carriers.
Fragile X syndrome is inherited in an X-linked pattern. Males have one X and one Y chromosome; females have two X chromosomes. This chromosomal difference largely explains why males frequently show more marked clinical features than females.
If a mother carries a premutation or full mutation, each child has a 50% chance of inheriting the affected X chromosome. Fathers with a premutation pass the altered X chromosome to all daughters but not to sons, who inherit the father’s Y chromosome. The number of CGG repeats can increase between generations (anticipation), so repeat size and risk should be reviewed in genetic counselling.
Some premutation carriers remain well but carry risks that may present later in life; these are discussed in the sections on prognosis and premutation-associated conditions.
Families with unexplained learning difficulties or developmental delay should be offered genetic counselling. The NHS provides diagnostic testing via specialised genetics services; a GP can arrange a referral for DNA analysis and discussion of reproductive options.
The FMR1 gene encodes the fragile X mental retardation protein (FMRP), which regulates synaptic function and neuronal connectivity. Insufficient FMRP disrupts communication between nerve cells and interferes with the formation of normal brain circuits.
Normal brain maturation relies on tightly regulated protein expression during sensitive developmental windows. Reduced FMRP alters synaptic development and plasticity, contributing to the learning, behavioural and sensory differences seen in fragile x syndrome.
Research into FMR1, FMRP function and downstream pathways remains active. Improved understanding of these molecular mechanisms informs development of targeted therapies and contributes to national and international research initiatives.
Fragile X syndrome causes a variable combination of physical, cognitive and behavioural features. Developmental concerns usually become apparent in early childhood; timely recognition of characteristic signs supports earlier diagnosis and access to therapies.

Facial and body features may be subtle in young children and become more distinct with age. Recognition of these features can prompt consideration of genetic testing as part of a wider developmental assessment.
Intellectual disability is a core feature in many affected males, ranging from mild learning difficulties to more significant impairment. Females commonly have milder cognitive effects because of their second X chromosome, though severity varies considerably.
Developmental delays typically appear in infancy or early toddlerhood. Parents often report delays in early motor skills, speech and social milestones compared with peers.
Behavioural differences commonly affect daily functioning. Clear understanding of these patterns helps families and clinicians plan effective management and support.
 Anxiety is common and can be triggered by social situations, noisy or crowded environments, and unexpected change. Effective strategies reduce distress and improve participation in everyday activities.
Anxiety is common and can be triggered by social situations, noisy or crowded environments, and unexpected change. Effective strategies reduce distress and improve participation in everyday activities.
Females with the full mutation often show a wide spectrum of effects. The second X chromosome provides partial protection for many, but around half of females with a full mutation may have an intellectual disability; presentation is highly variable.
Milder presentations in females commonly include learning difficulties and emotional or mental-health problems rather than pronounced physical features. This variability can delay recognition and diagnosis in some women.
Facial characteristics in females tend to be less obvious than in males. When concerns arise about development or learning, referral for genetic assessment is appropriate regardless of physical appearance.
Evidence shows that early intervention improves outcomes. Prompt referral for speech and language therapy, occupational therapy and behavioural support is recommended after diagnosis. For information about local services and to access early intervention pathways, families can contact The Fragile X Society.
There is a substantial overlap between fragile X syndrome and autism spectrum disorder (ASD). Around half of affected males and a smaller proportion of females meet criteria for ASD; the association makes fragile X syndrome one of the best characterised genetic contributors to autism.
Shared features include difficulties with social communication, repetitive behaviours and sensory sensitivities. Children with fragile x syndrome who also meet criteria for ASD may show different responses to interventions compared with those who have idiopathic autism, so assessment should guide individualised care plans.
Although many behaviours overlap, some differences can help clinicians and educators tailor support. Children with fragile x syndrome often retain a clear desire for social interaction but struggle with the mechanics of social exchange.
Patterns of eye contact may differ: brief eye contact followed by gaze aversion is commonly observed in fragile x syndrome, whereas other presentations of autism can show more persistent lack of eye contact. These patterns are not diagnostic on their own but can inform therapeutic approaches.
Sensory processing difficulties occur in both conditions and influence how children respond to therapy and educational strategies. Recognising the genetic basis of fragile x syndrome enables targeted adjustments to sensory and learning environments.
Symptoms of attention deficit hyperactivity disorder (ADHD) — notably hyperactivity, impulsivity and inattention — are common in fragile x syndrome and often appear in early childhood. These symptoms can compound learning and social challenges.
Males frequently present with more pronounced ADHD features than females. Medication may be helpful for some individuals but requires cautious selection and monitoring, since stimulants or other agents can exacerbate anxiety or behavioural symptoms in some people with fragile x syndrome.
Behavioural and environmental strategies are first-line for attention difficulties: structured routines, visual schedules and predictable transitions commonly reduce difficulties and support learning. Clinical teams should review medication effects closely and combine pharmacological with behavioural approaches where appropriate.
Accurate diagnosis depends on specialised genetic testing. Clinical concern arising from developmental delay, unexplained intellectual disability or a relevant family history should prompt consideration of testing for fragile X syndrome.
Testing is indicated when a child has developmental delays without an obvious cause, when there is a family history of fragile x syndrome or intellectual disability, or when females present with premature ovarian insufficiency. Testing is also appropriate for people with late-onset tremor and ataxia suggestive of fragile X-associated tremor/ataxia syndrome (FXTAS).
Diagnostic testing uses DNA analysis to determine the number of CGG repeats in the FMR1 gene. A blood sample is sent to a specialised genetics laboratory for analysis; results usually return within several weeks, though exact times vary by service and region.
The laboratory report distinguishes normal, intermediate, premutation and full mutation repeat ranges; each category carries different implications for diagnosis, prognosis and family counselling.
General practitioners can refer patients to regional genetics services for assessment and testing. Within the NHS, referrals to specialised genetics centres enable access to diagnostic testing and genetic counselling. Genetic counsellors explain the testing process, likely outcomes and implications for relatives.
Prenatal diagnostic options are available for families with a known carrier status. Chorionic villus sampling (CVS) or amniocentesis can identify FMR1 repeat size during pregnancy; these procedures carry small procedural risks that are discussed in detail during counselling.
Carrier testing identifies relatives who may pass the altered gene to their children. Siblings and prospective parents often choose testing to support informed reproductive decisions; results should be reviewed with a genetics professional.
A GP can arrange referral to local genetics services for fragile X syndrome testing. The NHS funds testing when clinical criteria are met. Waiting times vary by region, but genetic counselling appointments are generally offered within a matter of weeks. Contact the local genetics department or discuss referral with the GP to begin the testing pathway.
Laboratory results classify individuals by CGG repeat number; each category has specific clinical and family implications. The table below summarises the commonly used ranges and their significance.
| Category | CGG Repeats | Clinical Significance | Risk to Children |
| Normal | 5-44 | No symptoms expected | Low risk of expansion |
| Intermediate | 45-54 | Generally no symptoms | Small expansion risk |
| Premutation | 55-200 | Carrier status; possible risk of FXTAS or FXPOI | Risk of expansion when transmitted, depends on maternal status |
| Full Mutation | Over 200 | Associated with fragile X syndrome clinical features | If present in a mother, there is up to a 50% chance of passing the affected X to each child (varies by parental status) |
People with a premutation may develop fragile X-associated conditions later in life, such as FXTAS in some older adults or fragile X-associated primary ovarian insufficiency (FXPOI) in some females. These risks and their management are discussed in later sections and should be covered during genetic counselling and clinical review.
There is currently no cure for fragile X syndrome. Management aims to reduce symptoms, support development and optimise quality of life through coordinated, multidisciplinary care that addresses medical, educational and behavioural needs.

Specialist educational support is central to management. Individualised education plans should address cognitive strengths and difficulties and include adjustments to reduce sensory overload and anxiety.
Behavioural therapies assist with managing challenging behaviours and anxiety. Approaches such as positive behaviour support and other evidence-based behavioural programmes can teach alternative skills and reduce harmful behaviours. Where autism features are present, tailored interventions informed by specialist assessment are recommended.
Early referral for speech and language therapy is recommended for children with communication delays; many benefit from augmentative and alternative communication when spoken language is limited. Occupational therapy supports fine motor skills, daily living activities and sensory modulation. Physiotherapy can address gross motor delay and coordination.
Social skills programmes delivered in small groups or therapeutic settings help children practise interaction in a supported environment; techniques such as video modelling and role-play may be useful.
Medications are used selectively to target specific symptoms rather than the underlying genetic cause. Prescribing decisions should be personalised and closely monitored by healthcare professionals for benefit and side effects.
Stimulant medications can reduce hyperactivity and improve attention for some people; gradual dose titration and close monitoring are advised. Non-stimulant options are available for those who do not tolerate stimulants.
Selective serotonin reuptake inhibitors (SSRIs) or other anxiolytic strategies may be considered for persistent anxiety. Psychological and behavioural approaches should accompany any medication.
Seizures affect a minority of individuals (estimates commonly cited around 10–20%). Antiepileptic drugs control seizures for most people; neurology follow-up and regular review are important.
Some families explore complementary therapies such as music therapy or animal-assisted interventions; these may provide emotional or sensory benefits for some children. Evidence for dietary or supplement strategies remains limited and inconsistent.
Any complementary approach should be discussed with the healthcare team before starting to ensure safety and to avoid interactions with prescribed treatments.
The Fragile X Society provides practical guides on therapeutic approaches and can assist families in find experienced therapists. For therapy information and referrals, contact the Fragile X Society on 01371 875 100 or [email protected].
Most people with fragile X syndrome have a normal life expectancy. Longevity is not typically reduced by the condition, although long-term quality of life depends on symptom severity, coexisting conditions and the availability of appropriate support.
 Many people with mild to moderate features live independently or with minimal assistance; others require ongoing support for daily activities. Early intervention and sustained access to therapies and services contribute substantially to better long-term outcomes.
Many people with mild to moderate features live independently or with minimal assistance; others require ongoing support for daily activities. Early intervention and sustained access to therapies and services contribute substantially to better long-term outcomes.
Transitioning to adulthood brings specific challenges as educational services end and new arrangements for social care, employment and healthcare are required. Employment opportunities vary; supported employment and day programmes can provide structure and meaningful activity for many adults.
Living arrangements range from independent living with occasional support to residential care, depending on individual needs. Planning for transition should begin in adolescence and involve health, education and social-care teams to ensure continuity of support.
Healthcare needs continue across the lifespan. Regular medical review helps to identify and manage emerging problems. Mental-health support is important, as anxiety and depression may present or increase with age.
Structured social programmes, peer groups and supported activities help people build friendships and maintain wellbeing.
Certain medical issues are more common in people with fragile X syndrome; awareness and routine monitoring allow timely management.
| Condition | Frequency | Age of Onset | Management |
| Seizures | 10-20% of individuals | Childhood to adolescence | Antiepileptic medication |
| Heart Problems | 20% mitral valve prolapse | Any age | Cardiac monitoring |
| Vision Problems | Common | Childhood | Corrective lenses, monitoring |
| Ear Infections | Frequent in childhood | Early childhood | Antibiotics, tubes if needed |
| Sleep Problems | Very common | Any age | Sleep hygiene, medication |
Carriers of a fragile X premutation have distinct health risks. Fragile X-associated tremor/ataxia syndrome (FXTAS) affects a proportion of older male carriers and causes progressive tremor, balance problems and cognitive change.
Female premutation carriers may develop fragile X-associated primary ovarian insufficiency (FXPOI), which leads to irregular periods and earlier menopause in some women and may affect fertility. Regular specialist review helps to detect and manage these conditions promptly.
Families affected by fragile X syndrome often need specialised information, practical assistance and peer support. Several UK organisations provide dedicated resources, linking families and professionals to expert guidance and local networks.

The Fragile X Society is the principal national charity focused exclusively on fragile X syndrome. Founded in 1990 by families, the organisation provides comprehensive support across the UK for families and professionals.
The Fragile X Society offers free information, practical guidance and emotional support for families and healthcare professionals. Services include advisor support, newsletters, an online community, family weekends, conferences and multilingual resources. Contact the UK charity for specialist assistance.
Postal Address: The Chestnuts, 4 Stortford Road, Great Dunmow, Essex, CM6 1DA
Registered Charity Numbers: 1127861 (England & Wales), SC047332 (Scotland), Company No. 6724061
Several wider neurological and genetic charities provide complementary support, resources and local services for people affected by fragile x syndrome.
A UK charity supporting people with more than 600 neurological conditions, including fragile X syndrome. The Brain Charity offers counselling, group therapy, practical resources, social activities and carer support from its Liverpool centre and nationwide services.
Contact: 0151 298 2999
Email: [email protected]
Address: Norton Street, Liverpool, L3 8LR
Hours: Monday–Friday 9am–5pm
Cerebra supports children and young people aged 0–25 with brain conditions, including fragile X syndrome. The charity funds research (for example the BEOND study), produces information for families and runs support projects nationwide.
Focus: Children and young people 0–25 years
Services: Research, information, family support projects
The NHS provides fragile X syndrome testing and genetic counselling through regional genetics centres. A GP referral enables access to diagnostic testing, family screening and reproductive guidance.
Access: GP referral required
Coverage: NHS-funded when criteria met
Location: Regional genetics centres UK-wide
Specialist organisations offer information, emotional support, practical assistance and professional resources. Connecting with these services helps families navigate care pathways and access timely support.
Charities produce up-to-date guidance on the condition, available treatments and research developments. Educational materials help families and professionals understand genetic implications and management strategies.
Peer networks and helplines connect families with others who have similar experiences. Sharing practical advice and emotional support can reduce isolation and help with day-to-day problem solving.
Organisations assist with navigating healthcare, education and welfare systems. Practical help includes support with applications, referrals and local service information.
Healthcare and education professionals can access training, clinical guidance and referral information to support evidence-based care for people with fragile x syndrome.
Research into fragile X syndrome continues to expand understanding of its molecular basis and to evaluate potential treatments. Laboratory and clinical studies aim to translate knowledge of the FMR1 gene and its protein product into interventions that reduce symptoms and improve development.
Investigators are studying how loss or reduction of fragile X mental retardation protein (FMRP) alters neuronal function and synaptic connectivity. These studies identify downstream pathways that may be amenable to therapeutic modulation.
Gene-based approaches and other strategies to restore or compensate for FMRP function show promise in preclinical models. Translation into human therapy requires rigorous safety and efficacy testing; progress is incremental and carefully reviewed by regulatory and scientific bodies.
International funders, including specialist foundations and major bodies such as the National Institutes of Health, support basic and translational studies. National fragile X organisations also fund and co‑ordinate research and patient-centred initiatives.
Clinical trials have tested medications targeting specific neural systems; while some early-phase results were encouraging, larger studies have not always confirmed benefit. This highlights the complexity of developing treatments for genetic neurodevelopmental conditions and the need for robust trial design.
Current trials increasingly focus on early intervention, combination approaches and tailoring interventions to individual profiles. Ongoing studies examine whether treating during critical developmental windows produces greater functional gains.
Families and clinicians can support progress by participating in well‑designed studies. The Fragile X Society and other national organisations list UK research opportunities and clinical trial information. Participation helps build evidence while offering potential access to novel interventions under careful clinical oversight.
The Fragile X Society newsletter and charity communications provide regular updates on studies, trial openings and research reviews. Contact the society to join the mailing list and discuss whether research participation might be appropriate for a particular family.
Families and healthcare professionals commonly ask similar questions about fragile X syndrome. The answers below address key concerns and clarify practical points about diagnosis, prognosis and support.
Yes. Females with milder features are particularly likely to remain undiagnosed until adulthood, sometimes only identified when a child is tested. Adults with subtle learning difficulties or anxiety should be offered assessment and, if indicated, genetic testing.
Core developmental features are usually stable, but new challenges can arise at different life stages. Anxiety often increases in adolescence; premutation carriers may develop late-onset conditions such as FXTAS, which are distinct from childhood fragile x syndrome.
Estimates suggest fragile X syndrome affects about 1 in 4,000 males and 1 in 8,000 females in the UK. Carrier frequency is higher; around 1 in 250 females may carry a premutation. Check current national data for the latest figures.
Yes. Females show a wide range of outcomes. Approximately half of females with a full mutation may have intellectual disability, though severity varies due to X-inactivation and other factors; individual assessment is important.
No cure is available at present. Management focuses on therapies, educational support and targeted medical treatment for symptoms. Ongoing research aims to develop disease‑modifying treatments, but these are not yet established.
Fragile X syndrome is a genetic disorder that commonly causes intellectual disability and developmental delay and is classified as a learning disability under UK definitions. Individuals may also have physical, sensory and behavioural needs requiring multidisciplinary support.
Few public figures have disclosed a fragile X diagnosis, often for privacy reasons. Many families and advocates share personal stories via charities and support groups to raise awareness and provide peer support.
Not necessarily. Guidelines recommend testing when autism coexists with intellectual disability, a family history of learning difficulties, or physical features suggestive of fragile x syndrome. A clinician or genetic counsellor can advise whether testing is appropriate for an individual child.
Fragile X syndrome presents significant challenges for affected people and their families. A clear understanding of the genetic cause, early recognition of symptoms and timely access to appropriate support and therapies improve long‑term outcomes. Although the condition typically requires lifelong management, many individuals lead fulfilling lives with the right care in place.
 Early diagnosis enables interventions during critical developmental windows. Families benefit from connecting with specialised organisations for expert information and peer support. Healthcare teams play a central role in coordinating care, monitoring for associated health issues and arranging onward referrals.
Early diagnosis enables interventions during critical developmental windows. Families benefit from connecting with specialised organisations for expert information and peer support. Healthcare teams play a central role in coordinating care, monitoring for associated health issues and arranging onward referrals.
Research is ongoing into improved treatments and potential cures; participation in well‑designed studies helps advance knowledge for future generations. Progress is incremental and subject to rigorous scientific review.
Families are not alone in this journey. Thousands of UK families navigate similar challenges and can access national support through The Fragile X Society and partner organisations.
Whether newly diagnosed or experienced in managing fragile X syndrome, families can obtain practical and compassionate guidance from The Fragile X Society. Experienced advisors offer tailored information and connect members with a national network of families and professionals.
Contacting a specialist charity or the GP to request referral to genetics or local services is a helpful first step. Support, information and community connections make a meaningful difference.
Living with fragile X syndrome requires persistence, access to appropriate services and collaborative care from health, education and social‑care professionals. With comprehensive, compassionate support, each person with fragile x syndrome should be offered every opportunity to reach their full potential.
Book a personalised demonstration of the StandSure™ today by filling out our request form. Have any questions? Call us now, and our team will be happy to assist!



